 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
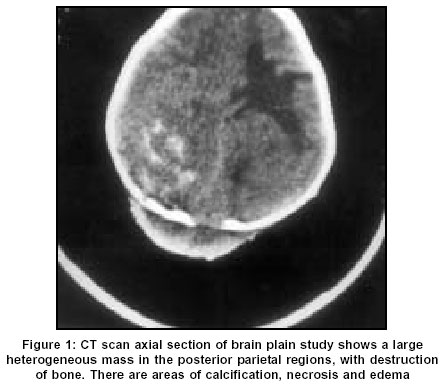
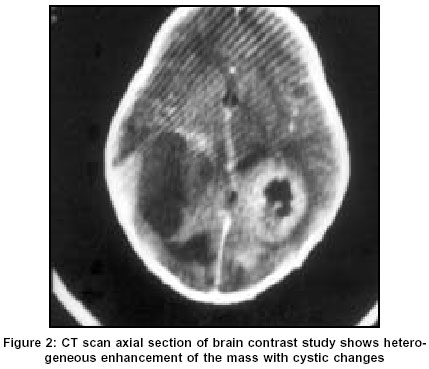
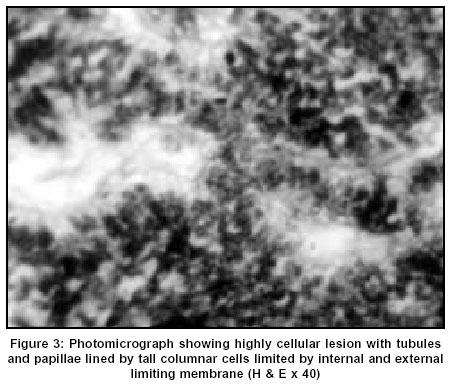
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 546-547 Case Report Medulloepithelioma: A case report Sundaram C, Vydehi BV, Reddy JJ, Reddy AK Departments of Pathology, Nizam’s Institute of Medical Sciences, Hyderabad Code Number: ni03175 Abstract Histological, immunohistochemical, and CT morphological features of medulloepithelioma, a rare embryonal tumor of primitive neuroepithelium, are described. Introduction Cerebral medulloepithelioma is a rare pediatric embryonal neuroepithelial tumor of the central nervous system (CNS). Histologically, medulloepithelioma recapitulates a primitive neural tube and displays multiple lines of differentiation including neuronal, glial and mesenchymal elements.[1],[2] It carries dismal prognosis with a median survival of 5 months.[3] We report imaging and pathological features of a cerebral medulloepithelioma in a child. Case Report A 3-year-old male child presented with swelling of the scalp in the occipital region and loss of vision of 2 months duration. Examination showed an emaciated child. The mass measured 8 x 4 cm and was non-pulsatile. It was firm in consistency with cystic areas and the skin over the swelling was free. There was no ulceration. The mass rapidly increased in size in the few weeks that he stayed in the hospital. Contrast CT scan of the brain showed a heterogeneously enhancing lesion in the occipito-parieto-temporal region involving both the hemispheres, with perilesional edema. It showed areas of necrosis and calcification [Figure - 1] & [Figure - 2]. There was destruction of the occipital bone with extension of the mass into the subcutaneous planes. Hematological investigations, blood biochemistry, and ultrasound of the abdomen were normal. Fine needle aspiration cytology showed a round cell tumor. Open biopsy with debulking of the mass was done. Postoperatively, the patient's condition deteriorated and he succumbed. A partial autopsy limited to examination of the brain was carried out. At autopsy, the brain, with a large fleshy tumor measuring 12 x 10 x 8 cm in the occipito-parieto-temporal region involving both the cerebral hemispheres, was removed. There was a defect in the occipital bone through which the mass was extending into the subcutaneous planes. The meninges were dull in color. There was bilateral tonsillar herniation and distortion of vessels of the circle of Willis. The lesion was gray white, fleshy with large areas of hemorrhage, necrosis and calcification. The skull bone was infiltrated by the tumor. The cerebellum and brainstem were normal. Microscopically, there was a dense cellular lesion with large areas of necrosis. The cells were columnar, arranged in compact tubules and papillae. The cells showed pseudo-stratification with an external and internal limiting membrane, resembling a primitive neural tube [Figure - 3]. There were 2-3 mitoses per high power field. There was marked pleomorphism. There were sheets of undifferentiated cells in other areas. There was no neuronal, glial or mesenchymal differentiation. By immunohistochemistry the tumor cells were not labeled by antibodies to GFAP, NSE, vimentin, desmin and epithelial membrane antigen indicating the undifferentiated nature of the tumor. Discussion Medullary epithelioma is an extremely rare, highly malignant primitive embryonic tumor apparently derived from the primitive medullary plate and neural tube. Bailey and Cushing originally classified the tumor in 1926[4] as the most primitive neoplasm of the CNS. Rorke et al[5] classified this tumor into two subtypes: i) medulloepithelioma not otherwise specified ii) medulloepithelioma with differentiation into astrocytes, oligodendrocytes; ependymal cells; neuronal cells; others (melanin, mesenchymal cells); and mixed cellular elements. These are essentially tumors of childhood with the age of onset between 6 months and 5 years, though congenital tumors and the occurrence of the tumor beyond this age range has also been described.[2],[6],[7] There is no specific sex predilection.[3] The reported sites include cerebral hemispheres, brainstem, cerebellum, and peripheral sites.[3],[4],[8],[9] The common site is periventricular involving temporal, parietal, occipital and frontal lobes and also the posterior fossa.[1],[3],[8],[9],[10],[11],[12] The periventricular location suggests origin from primitive undifferentiated matrix cells. On non-contrast CT scan the lesion is either isodense or hypodense with variable heterogeneity and calcification. The tumor enhances with contrast.[3] Such neuroimage features should suggest primitive neuroectodermal tumor, more so in children. Few studies are available regarding the immunohistochemical profile of medulloepitheliomas.[3],[12] It is noted that neural tube-like structures are positive for vimentin in the majority of the tumors. However, in our patient the cells were not positive for vimentin as well as for other markers, thus suggesting that it was medulloepithelioma with poor differentiation. The optimal course of management of medulloepithelioma is unknown. Gross-total resection followed by radiation therapy is often the mode of treatment.[3] Radiotherapy alone was associated with prolonged survival in 2 cases.[3] The case under study had a fatal outcome due to extensive brain involvement. The utility of aggressive chemotherapy including autologous bone marrow transplant warrants further investigation. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=546;epage=547;aulast=Sundaram The following images related to this document are available:Photo images[ni03175f2.jpg] [ni03175f3.jpg] [ni03175f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}