 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
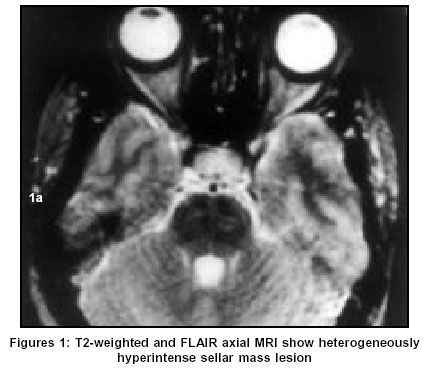
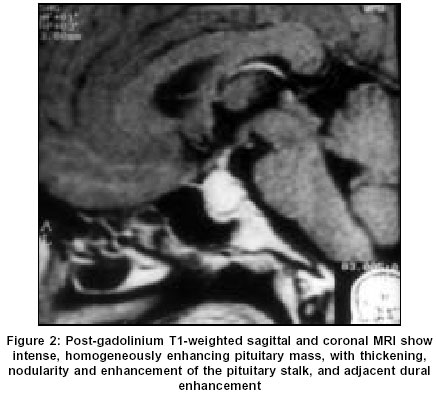
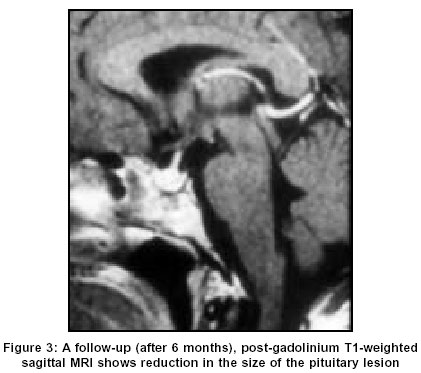
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 548-550 Case Report Pituitary tuberculoma: Magnetic resonance imaging Singh S Department of Radiodiagnosis and Imaging, Christian Medical College and Hospital, Vellore - 632004 Code Number: ni03176 Abstract A case report of a pituitary tuberculoma, with magnetic resonance imaging (MRI) features is described. The patient was treated with anti-tuberculous chemotherapy, and a follow-up MRI after 6 months showed good response. The relevant literature is briefly reviewed.Introduction Intracranial tuberculosis is responsible for 0.15% of intracranial space-occupying lesions in developing countries.[1] Computed tomography (CT) and magnetic resonance imaging (MRI) features have been described in a few cases of sellar tuberculoma. Most of the cases reported showed suprasellar and parasellar involvement. A few reported cases were purely intrasellar in location, which can simulate adenoma with or without hormonal dysfunction.[2],[3],[4],[5] Pituitary tuberculoma can present as an isolated central nervous system lesion, without systemic involvement.[1] As in the present case, the diagnosis of all the previously reported cases was established on histopathological examination of the excised specimen.Case Report A 34-year-old woman presented with history of headache and vomiting of 5-month duration, and galactorrhea and amenorrhoea of 2-month duration. The other relevant history, and neurological (including eye) as well as physical examinations were normal. The prolactin level was 85 ng/ml (normal 2-15ng/ml). Other hormonal levels, cerebrospinal fluid and routine blood tests were normal. MRI showed a well-defined sellar mass with mild suprasellar bulge, measuring 2.5 x 1.8 x 1.5 cm in size. On T1-weighted images, the mass was isointense to gray matter, and on T2-weighted imgaes including fluid attenuated inversion recovery (FLAIR), heterogeneously hyperintense [Figure - 1]. The post-gadolinium images showed moderate to marked homogeneous enhancement of the mass, pituitary stalk and surrounding dura. The stalk showed thickening and nodularity [Figure - 2]. Initial diagnosis of pituitary tumor was considered. The patient had bromocriptine intolerance; hence, transnasal transphenoidal excision of the pituitary mass was performed. Per-operatively, the sellar mass was firmly and densely adherent to the surrounding structures, and vigorous dissection could have injured surrounding structures, therefore, it was incompletely excised. Histopathologically, the excised specimen (paraffin block) showed dense aggregates of lymphoid cells with occasional plasma cells around a few granulomas composed of epithelioid cells and Langhans' type multinucleated giant cells. These findings were consistent with pituitary tuberculoma. Acid-fast bacilli were not present on Zeihl-Neelsen staining. The fungal and bacterial cultures were negative. The patient was treated with anti-tuberculous drugs, with good clinical response (normal menstrual cycle, no galactorrhea, reduced headache and vomiting, and prolactin level: 6.0 ng/ml). A follow-up MRI (after 6 months) showed reduction in the size of the pituitary lesion (1.6 x 1.5 x 1.2 cm) [Figure - 3].Discussion Pituitary tuberculoma, as an isolated manifestation of the disease is a very rare entity.[1],[5],[6] Isolated sellar tuberculoma, without extracranial tuberculous focus, although not unusual is intriguing.[4],[6] Clinically, they may present as hormonal secreting/ or non-secreting masses mimicking adenomas.[1],[5] The clinical features of endocrinopathy may or may not be present, and mild to moderate hypopituitarism may be detected in asymptomatic patients.[1],[6],[7],[8],[9] The patient may have profound hypopituitarism with a relatively small mass lesion.[4] Majority of the reported cases of intrasellar tuberculoma were in adult females.[4] It can result from hematogeneous spread, or, directly from the infection of the cranial base.[1] Radiologically, they present as a sellar mass similar to pituitary adenoma. Thickening, nodularity and enhancement of the pituitary stalk and infundibulum have been reported as findings suggestive of tuberculoma.[1],[3],[6],[8] However, they are non-specific findings and can also occur in other diverse conditions like neoplasms, inflammatory diseases such as sarcoidosis, syphilis, granulomatous hypophysitis, and eosinophilic granuloma.[1],[7],[10] Thickening of the stalk is also seen in association with tuberculous meningitis. In the present case, there was no clinical suspicion of an infectious pathology. The lesion was predominantly intrasellar with a suprasellar bulge. It was heterogeneously hyperintense to white matter on long TR-weighted images, and isointense on short TR-weighted images. On post-gadolinium images, there was intense enhancement. The images showed thickening, nodularity and enhancement of the pituitary stalk and infundibulum, and also adjacent dural enhancement. These findings could have given us a clue to suspect a granulomatous lesion.[5] Because of the rarity of pituitary tuberculoma, it was not considered and excision biopsy revealed the mass to be a pituitary tuberculoma. In developing countries, where tuberculosis remains endemic, the diagnosis of pituitary tuberculosis is more likely for sellar lesions with a thickened nodular enhancing pituitary stalk and infundibulum, and surrounding dural enhancement.[1],[5],[6] Pereira et al reported a case with enlarged hypophysis with a non-enhancing intrasellar isointense lesion, and thickening of the infundibulum and the pituitary stalk.[1] Sinha et al reported an intrasellar mass lesion with suprasellar bulge, which was heterogeneously hyperintense to white matter on T2-weighted images, and isointense on T1-weighted images, with intense enhancement and a focal hypointense area on the left side of sella, adjacent to the sellar floor, and thickening and enhancement of the pituitary infundibulum and stalk.[6] Navnit et al also reported a case with MRI features of thickening and enhancement of the stalk and surrounding dura.[5] There was a variable signal characteristic of the pituitary tuberculoma on long TR-weighted images, heterogeneously hyperintense to white matter in two,[1],[5] and homogeneously hyperintense in one patient.[6] However, the lesions were isointense on T1-weighted images.[1],[5],[6] CT findings in 5 cases of sellar tuberculoma with suprasellar extension and hyperdense dense enhancement have been described.[8] One patient had basal enhancing exudates suggesting associated tuberculous meningitis.[8] In conclusion, a rare case of an isolated pituitary tuberculoma may be difficult to diagnose clinico-radiologically. The post-gadolinium MRI features of nodular thickening and enhancement of the stalk and infundibulum can give a clue to the diagnosis. Early recognition of a possible pituitary tuberculoma can help in treating the patient conservatively, with fewer hazards than operative intervention. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=548;epage=550;aulast=Singh The following images related to this document are available:Photo images[ni03176f3.jpg] [ni03176f2.jpg] [ni03176f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}