 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
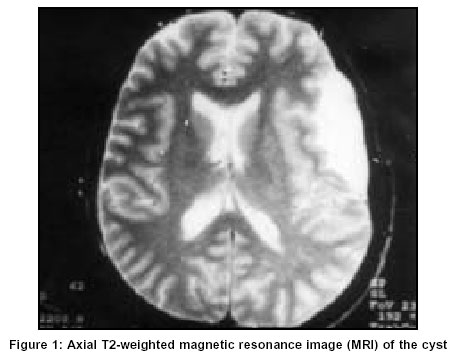
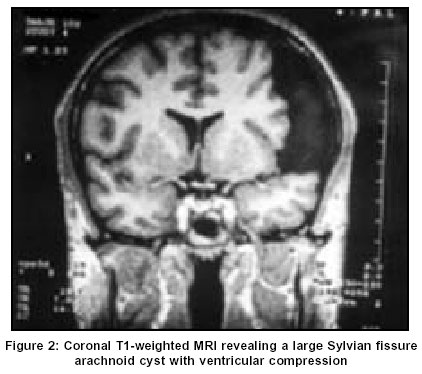
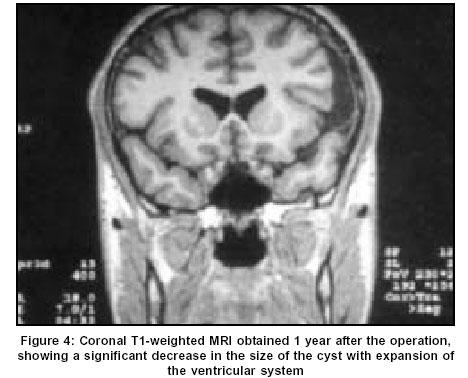
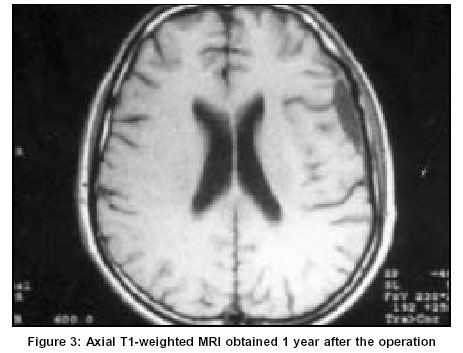
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 553-554 Short Reports Tapping of a type II sylvian fissure arachnoid cyst: Technical note Pierangeli E, Gigante N, Pizzoni C U.O. di Neurochirugia A.O. “SS. Annunziata”, Via Bruno,
74100, Taranto Code Number: ni03178 Abstract A 28-year-old man with a large Sylvian fissure cyst was treated by making a small pre-coronal burr hole, and subsequently, under a direct view its wall was fenestrated with a Cushing’s needle and the cyst fluid was tapped. The patient had complete neurological recovery. The follow-up was of 90 months. Introduction Arachnoid cysts are benign lesions and account for 1% of all non-traumatic intracranial masses.[1],[2] They are congenital lesions, and contain clear, colourless liquid resembling normal cerebrospinal fluid. Despite several studies, their mechanism of formation is not completely understood.[3] Cysts of Sylvian fissure are the most frequent (about 49 to 65.2 % of all intracranial arachnoid cysts). There is a higher incidence in males and a left side preference.[4] Many surgical techniques for the therapy of symptomatic arachnoid cysts have been suggested: cysto-peritoneal shunting, cyst excision, cyst fenestration, cystocisternostomy, ventriculocystostomy and stereotactic aspiration; nevertheless, the choice of the best method of treatment remains controversial.[2] We describe an alternative method of treatment of an arachnoid cyst. Case Report A 28-year-old man presented with a history of diplopia, repeated episodes of headaches and disturbed sleeping patterns for 10 days. He had a transient episode of double vision 5 years ago. MRI revealed the presence of a wide (about 7 x 2.5 x 2.5 cm) Sylvian cyst that caused displacement of the adjacent cranial theca and atrophy of the surrounding cerebral tissue [Figure - 1] & [Figure - 2]. Because the cyst was large (Type II according to the classification of Galassi et al[5]) and symptomatic, a surgical treatment was considered. Under local anesthesia, a small left pre-coronal burr hole was made about 6 cm from the midline and the dura was opened. The outer cyst membrane was perforated with a Cushing's needle, and then a small catheter was inserted into the cyst with an up and down movement to enlarge the cyst fenestration. The cystic fluid was tapped through the same catheter. The catheter was left in the cyst for about 20 minutes during which time the valsalva maneuver was performed on multiple occasions. After the operation the double vision disappeared completely in 2 months. The headaches also disappeared completely in the following months. The sleep pattern became regular, and he resumed regular work as an army officer. Post-procedure MRI showed progressive reduction in the size of the cyst [Figure - 1] & [Figure - 4]. Discussion Symptomatic arachnoid cysts are generally treated either by removal or fenestration of the external wall of the cyst, after open craniotomy or by cystoperitoneal shunting[2],[6] assuring drainage of the cyst content. However, although simple, these procedures are not free from complications like relapse, chronic subdural hematoma due to bleeding of bridging veins passing along the cyst wall, obstruction owing to coalescence of the cyst wall, and infections.[7],[8] Currently, endoscopic cyst evacuation and cyst wall fenestration is the treatment of choice for arachnoid cysts.[2],[9] We successfully performed a left pre-coronal burr hole that enabled a direct vision of the cyst wall due to its superficial location. The cyst wall was perforated safely, avoiding the risk of injuring vessels or other surrounding structures. With our experience in this case, we believe that the arachnoid cyst fluid absorption occurs if a communication (even small) between the cystic space and the subdural space is made. This is probably due to differences in osmotic pressure between the cystic space and subdural space which facilitate the outflow of cystic fluid and consequently the reduction of the cyst.[10] We feel that for superficial arachnoid cysts, a simple burr hole exposure and wide fenestration of the cyst wall can be a useful modality of treatment. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=553;epage=554;aulast=Pierangeli The following images related to this document are available:Photo images[ni03178f2.jpg] [ni03178f3.jpg] [ni03178f4.jpg] [ni03178f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}