 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
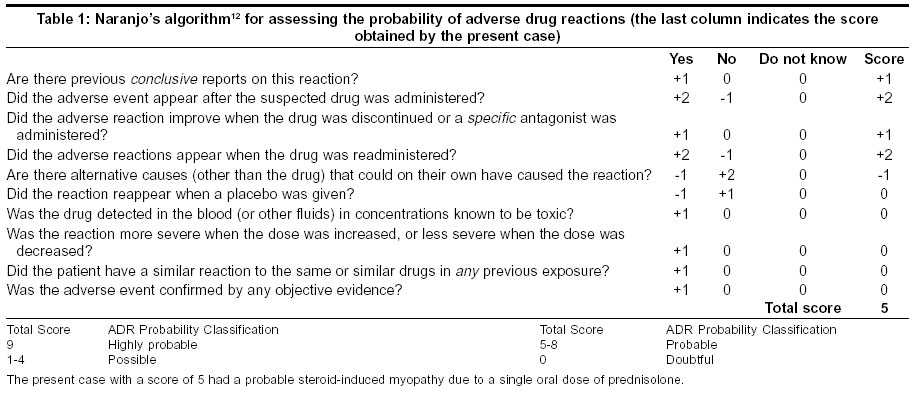
Neurology India, Vol. 51, No. 4, October-December, 2003, pp. 554-556 Short Reports Steroid-induced myopathy following a single oral dose of prednisolone Kumar S Neurology Unit, Department of Neurological Sciences, Christian Medical College Hospital, Vellore - 632004, Tamil Nadu Code Number: ni03179 Abstract This report describes a case of acute steroid-induced myopathy following a single dose of oral prednisolone. A 55-year-old man presented with an acute exacerbation of chronic obstructive pulmonary disease (COPD), which was treated with prednisolone 40 mg daily in addition to bronchodilators. He developed features of myopathy the next day. Serum CPK was moderately elevated and electromyogram (EMG) was suggestive of primary muscle disease. He was managed conservatively and improved 10 days after stopping prednisolone. Mechanisms of steroid-induced myopathy and relevant literature have been reviewed. Introduction Cushing first described steroid-induced myopathy in 1932. Two different clinical patterns of this condition are seen-chronic and acute.[1] The chronic form is more common and occurs after prolonged usage of oral corticosteroids.[2] The acute form is uncommon and occurs after administration of large doses of intravenous corticosteroids.[3],[4],[5],[6] Acute myopathy following administration of a single low dose of parenteral triamcinolone has also been reported.[7] This report describes a patient who developed features of steroid-induced myopathy after administration of a single dose of oral prednisolone, given for acute exacerbation of chronic obstructive pulmonary disease (COPD). Case Report A 55-year-old man presented with features of acute exacerbation of COPD. He was a known case of COPD for 9 years on treatment with oral deriphylline and inhaled salbutamol. On examination, he had a respiratory rate of 35 breaths per minute and was using accessory muscles of respiration and the pulse rate was 92 beats per minute. Auscultation of the chest revealed bilateral wheeze. He was started on nebulized terbutaline, oral deriphylline 200 mg thrice daily and prednisolone 40 mg once daily. He was also given oxygen by nasal prongs. The patient was not given antibiotics or sedatives. He showed a good response and became comfortable within 3 hours of admission. The following morning, the patient complained of difficulty in getting up from the squatting position and inability to walk without support. He also complained of myalgia. He had no sensory or bladder symptoms. On examination, power was grade 3 in the upper limbs and grade 2 in the lower limbs proximally. Distal power was grade 4/5 (Medical Research Council grading). There was no clinical involvement of the respiratory, neck and oculopharyngeal muscles. Sensory examination and deep tendon reflexes were normal. Plantars were flexor. The hematological examination revealed no abnormality. Nerve conduction studies were normal. Serum CPK was 857 U/L. In the meanwhile, the patient had received another dose of prednisolone 40 mg the following day and his condition had worsened to a state where he was unable to get up from the supine position. A possible diagnosis of steroid-induced myopathy was considered at this stage [Table - 1] and prednisolone was stopped. Subsequently, the patient started to improve and was able to walk within 2 days. He reached his premorbid level of functioning within 10 days of stopping prednisolone. Repeat CPK at the time of discharge was 118 U/L. The patient has since been followed up for 6 years and has not had a recurrence of his weakness. Discussion Steroid-induced myopathy occurs more commonly with chronic usage of fluorinated steroids (such as dexamethasone or triamcinolone) as compared to non-fluorinated ones (such as prednisolone or hydrocortisone).[1] A sedentary lifestyle may increase the risk of muscle weakness in a patient taking corticosteroids as less active muscles are preferentially affected in this condition. Women are affected twice as commonly as men. The exact mechanism of the muscle weakness is unclear but may be related to decreased protein synthesis, increased protein degradation, hypokalemia, and/or decreased sarcolemmal excitability.[8] Growth hormone and insulin-like growth factors-I (by decreasing the steroid-induced glutamine synthetase activity) have been found to have preventive effects on myopathy due to steroids.[9],[10] There are no specific laboratory findings in steroid-myopathy.[9],[10] Serum CPK and LDH are usually normal or mildly elevated.[11] An elevated urinary creatine excretion, if found, may be specific for this condition.[10],[11] EMG may be normal in the early phase but shows features of muscle disease later in the course.[4] Muscle biopsy done in the chronic form shows preferential type II fiber atrophy, whereas both types of fibers (type I and II) are affected in acute myopathy.[1],[10] However, a diagnosis is often made without resorting to muscle biopsy.[11] As type II muscle fibers are used for high-intensity, low-endurance activities, such as sprinting, these activities are impaired in chronic steroid myopathy as type II fibers are preferentially affected. In conclusion, it is important to keep in mind a possibility of steroid myopathy in a patient who develops acute weakness after starting oral or parenteral steroids. References
Copyright 2003 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2003;volume=51;issue=4;spage=554;epage=556;aulast=Kumar The following images related to this document are available:Photo images[ni03179t1.jpg] |
| |||||||||

{kind=link}