
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 1, 2004, pp. 43-53
|
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 43-53
Review Article
Vein of galen malformations: Review
Gupta AK, Varma DR
Department of Radiology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum - 695011
Correspondence Address:Department of Radiology, Sree Chitra Tirunal
Institute for Medical Sciences and Technology, Trivandrum - 695011 gupta@sctimst.ac.in
Code Number: ni04012
Abstract
Vein of Galen malformations are unique congenital malformations of the
cerebral vasculature that result in persistence and ‘aneurysmal’ dilatation
of the venous structures. The varied clinical presentations and their distinctive
and complex angioarchitecture make it important for the caring physician
to understand their embryological and pathophysiological aspects. Management
of these lesions – both in the neonatal period and at the time of definitive
intervention, is challenging. Considering the rarity of these lesions,
there are very few studies that have been able to compare the results of
different techniques in the management. Continuing developments in the
diagnostic as well as interventional aspects during the last two decades
have radically changed the management of these lesions. Antenatal diagnosis
and referral to a center with facilities for advanced neonatal cardiac
care as well as for interventional neuroradiological therapy can go a long
way in improving the prognosis in these children.
Introduction Vein of Galen malformations (VOGMs) are rare anomalies of intracranial circulation that constitute 1% of all intracranial vascular malformations. However, they represent 30% of vascular malformations presenting in the pediatric age group.[1] These lesions are characterized by the presence of an aneurysmally dilated midline deep venous structure, fed by abnormal arteriovenous communications.
Steinheil in 1895, made the first reference to a Galenic malformation-referring
to it as a ′varix aneurysm′.[2] Since
then, these lesions have been variably referred to as ′aneurysms of the vein of Galen′, ′arteriovenous aneurysms of the vein of Galen′, ′vein of Galen aneurysmal malformations′ and ′vein of Galen malformations′. The nomenclature is imprecise because the dilated venous structure that is characteristic of these malformations has been demonstrated to represent the embryonic median prosencephalic vein, and not the vein of Galen.
Though these lesions are extremely uncommon, they are of special interest
to the interventional neuroradiologist because endovascular therapy has
proved itself to be an effective, and often the only safe therapeutic
modality available to treat these patients.
Embryology Since VOGMs represent embryonic vascular malformations, they are associated with the persistence of vascular arrangements that are characteristic of a particular period of development. A sound knowledge of the embryology of the cerebral vasculature is essential to understand the angioarchitecture and pathophysiological features that are unique to these lesions. Raybaud and co-workers were the first to recognize that the ectatic venous structure that is characteristically seen in these lesions represented the median prosencephalic vein and not the vein of Galen itself.[3]
The development of cerebral vasculature can be divided into three stages.
During the first phase of ′extraembryonal supply′, the
open neural tube is nurtured by the amniotic fluid that surrounds it.
The phase of ′extrinsic vascularization′ is characterized
by the presence of a highly vascularized neural crest derivative known
as ′meninx primitiva,′ which surrounds the neural tube.
Nutrients are transported from this cellular connective tissue to the
neural tube by diffusion. Small capillaries form within this tissue,
which unite in the more superficial layers and form a network of arteries
and veins. The third phase of ′intrinsic vascularization′ is
characterized by the development of blood vessels within the cerebral
parenchyma.[3],[4]
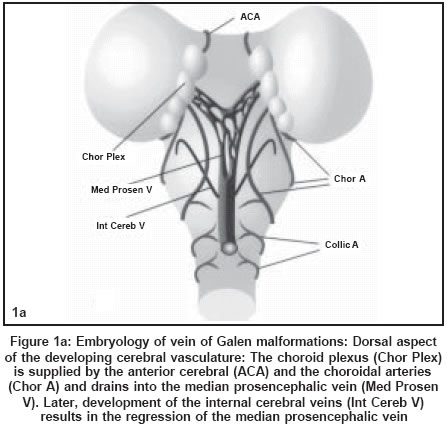
The primary abnormality that is responsible for the development
of vein of Galen malformations occurs after the stage of the 21-23 mm
embryo [Figure - 1 a, b]. By that time, the primary internal carotid
artery and its terminal branches-the anterior cerebral and anterior choroidal
arteries have formed. Apart from supplying the developing telencephalic
vesicles, these arteries also supply the area epithelialis in the region
of the roof of the third ventricle, which later evolves into the choroid
plexus. The internal carotid artery also supplies the hindbrain through
the posterior communicating artery, from which originate the early posterior
choroidal and mesencephalic arteries. Simultaneous growth of the collicular
plate results in the development of the quadrigeminal arteries.[3]
Development of the telencephalic choroid plexus is accompanied by simultaneous differentiation of a transient venous structure on the roof of the diencephalon. This venous structure drains the choroid plexuses and has been designated as the median prosencephalic vein or the primitive internal cerebral vein. By the 11th week (50-mm embryo), the development of the basal ganglia results in the formation of the paired internal cerebral veins, which annex the venous drainage of the choroid plexuses. This results in the regression of the median prosencephalic vein, except for its most caudal part, which joins the internal cerebral veins to form the vein of Galen.[3]
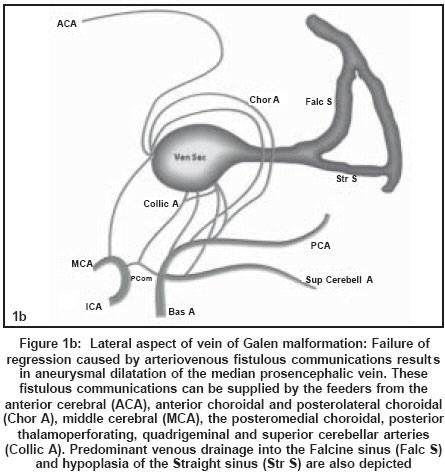
Vein of Galen malformations arise as a result of direct arteriovenous communications
between the arterial network and the median prosencephalic vein. Based
on the angioarchitecture of these lesions, Raybaud and co-workers concluded
that the insult causing this abnormal development occurs between the
6th and 11th week of intrauterine life.[3] The
arteriovenous communications occur within the cistern of velum interpositum
and the quadrigeminal cistern. The principal feeders of the malformation
are those that normally supply the tela choroidea and the quadrigeminal
plate. These include the anterior or prosencephalic group (the anterior
cerebral, anterior choroidal, middle cerebral and the posterolateral
choroidal arteries), and the posterior or mesencephalic group (the posteromedial
choroidal, posterior thalamoperforating, quadrigeminal and superior cerebellar
arteries).[1],[3] The
median prosencephalic vein, which drains the shunt, lacks a fibrous wall
and is largely unsupported. It lies free in the subarachnoid space within
the cistern of velum interpositum and therefore it balloons out to a
large size. The high flow across the arteriovenous fistula may result
in the retention of fetal patterns of venous drainage. Persistence of
the falcine sinus, which is a transient embryonic structure that connects
the straight sinus to the superior sagittal sinus, is one such association.
Retention of fetal patterns of venous drainage could prevent development
of other sinuses such as the straight sinus. Retention of the embryonic
pattern of vasculature can explain the presence of several vascular anomalies
that are associated with these lesions.[3],[4]
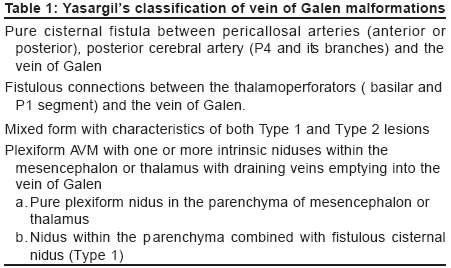
Classification There have been several attempts to classify VOGMs. The two most widely used classification systems have been provided by Yasargil and Lasjaunias. Yasargil classified VOGMs into four categories [Table
- 1].[5] Type 1, 2 and 3 lesions in Yasargil′s classification involve a direct fistulous communication with the vein of Galen. There is no other proximal nidus. Type 4 lesions represent parenchymal arteriovenous malformations (AVMs), which drain into the vein of Galen. Yasargil described that angiographic differentiation of Type 4 lesions from the other types is based on the appearance of veins draining the AVM (internal cerebral vein, median atrial vein or basilar vein) during the arterial phase of the angiogram.
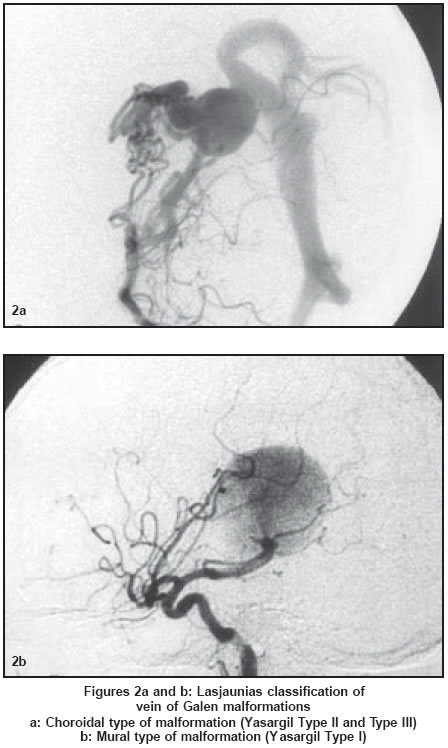
VOGMs have been classified by Lasjaunias and colleagues into choroidal
and mural types depending on the location of the fistula [Figure
- 2].[4],[6] Multiple
fistulas communicating with the anterior end of the median prosencephalic
vein characterize choroidal type malformations. This type of malformations
is supplied by the choroidal, subforniceal or pericallosal arteries or
by subependymal branches of thalamoperforators. In mural type malformations,
the fistula is located in the wall (usually in the inferolateral margin)
of the median prosencephalic vein. The collicular and posterior choroidal
arteries usually supply the shunt.
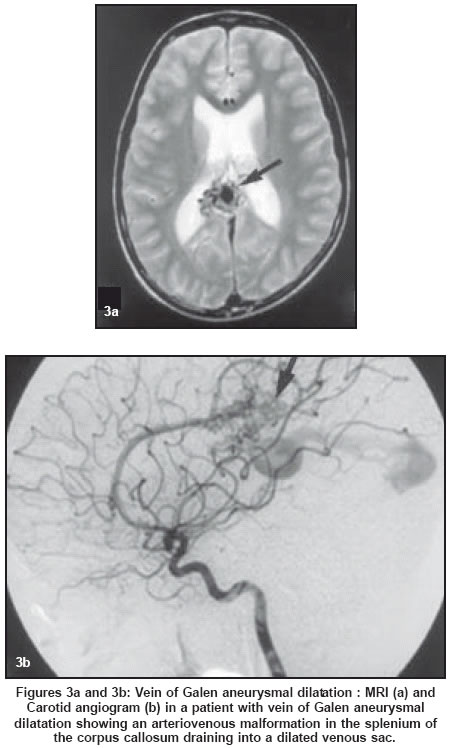
These types should be differentiated from the vein of Galen aneurysmal
dilatation [Figure - 3],
which represents dilatation of a normally formed vein of Galen, secondary
to outflow obstruction. In this form, the dilated venous structure
drains a parenchymal AVM as well as the normal cerebral parenchyma.[6],[7] These
patients present in childhood or early adulthood, with features of
hemorrhage, seizures and focal neurological deficits.[4]
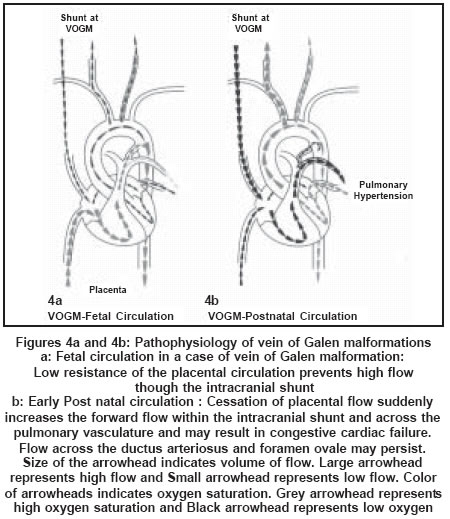
Pathophysiology Cardiac manifestations
During intrauterine life, the low resistance of the placental circulation competes with the cerebral arteriovenous shunt, thereby blood flow through the shunt is not as great as it is after birth [Figure:4a]. The left ventricle supplies the fistula while the right ventricle supplies the placenta and the rest of the body. Thus, the circulatory overload is shared between the two ventricles, which work in parallel.[8]
After birth, each ventricle supplies the entire circulation in series.
Thus, the burden on each ventricle increases and cardiac failure ensues.
Exclusion of the low resistance placental circulation results in an abrupt
increase in the flow across the fistula [Figure:4b]. As much as 80% of
the left ventricular output may be supplied to the brain in severe cases.
This necessitates a compensatory increase in the cardiac output and blood
volume to maintain perfusion of the systemic vasculature. This excessive
flow across the pulmonary vasculature results in pulmonary hypertension.
Increased venous return to the right atrium promotes right-to-left shunting
through the patent foramen ovale. Right-to-left shunting also occurs
at the level of the ductus arteriosus, which remains patent due to the
rise of pulmonary arterial pressure above the systemic pressure. These
right-to-left shunts are responsible for the cyanosis that may occur
in these patients. Large arteriovenous shunts significantly reduce the
diastolic pressure within the aorta, causing reduced coronary artery
flow. The increased cardiac output results in high ventricular intracavitary
pressure. Both these factors are responsible for the reduction of the
subendocardial blood flow, thereby promoting myocardial ischemia.[8],[9],[10]
Thus, the cardiac failure in neonates with VOGMs is multi-factorial in origin and is usually refractory to medical management.
Neurological manifestations
Cerebral venous hypertension is the etio-pathogenetic factor that is responsible for most neurological manifestations of VOGMs. These lesions are usually associated with venous anomalies in the form of poorly developed venous drainage or secondary venous stenosis and occlusion. The high flow within the arteriovenous shunt and restriction of venous drainage results in high cerebral venous pressure. In infants, as the arachnoid granulations have not yet fully matured, most of the ventricular CSF is reabsorbed across the ventricular ependyma, into the brain parenchyma, for subsequent drainage by the medullary veins. In infants with VOGMS, the high venous pressure transmitted to the medullary veins prevents resorption of fluid and thus results in hydrocephalus, cerebral edema, and hypoxia.[11] Thus, hydrocephalus is secondary to impaired resorption of CSF due to venous hypertension and not due to aqueductal compression.[12],[13] The chronic hypoxia produced by the venous hypertension results in progressive cerebral parenchymal damage resulting in cognitive impairment, which can range from delayed milestones to mental retardation.[4],[14]
The
fistula may be drained by rerouting its blood flow into the cavernous
sinus and further into the facial veins or basilar or pterygoid plexus.
These collateral pathways of venous drainage account for the prominence
of facial venous channels, which is commonly seen in infants with VOGMs
and also for the occasional case that presents with epistaxis.[4],[15]
Clinical presentation
Gold et al in 1964 provided a clinical classification system for VOGMs that remains valid today.[16] They correlated the age at presentation with the clinical presentation and pathophysiology and described three characteristic groups of patients.
Neonates
Neonates characteristically have multiple fistulas. Up to 25% of their cardiac output passes through the fistulas causing high-output congestive cardiac failure. Depending on the size of the shunt, adequacy of venous drainage, complexity of arterial supply and the host response, the cardiac manifestations can range from asymptomatic cardiomegaly to severe cardiac failure that is refractory to medical management. Cyanosis may be seen in these patients and the presentation may be mistaken for congenital cyanotic heart disease.[17] Features of myocardial ischemia may be detected on electrocardiography.[4],[8],[18],[19] Infants and children
Infants and children usually have a single fistula with a smaller shunt. Cardiac manifestations are absent or very mild. These patients present with macrocephaly or with hydrocephalus. Patients with longstanding cerebral venous hypertension may also present with delayed milestones. A high proportion of these children present with failure to thrive. Though this could be due to cardiac decompensation, hypothalamic and hypophyseal dysfunction secondary to venous congestion must also be considered as a potential mechanism.[4],[20] Older children and adults
Older children and adults usually have low-flow fistulae. These patients usually present with headache and seizures. A small number of patients may also present with developmental delay, focal neurological deficits, proptosis and epistaxis. Subarachnoid hemorrhage and intracerebral hemorrhage can occur in this age group due to rerouting of blood into the pial veins.[4] Imaging
The widespread use of routine antenatal ultrasonographic examinations has enabled the detection of several cases of VOGMs in the third trimester of pregnancy.[21],[22],[23],[24] Apart from identification of the abnormality and its differentiation from other nonvascular space-occupying lesions, ultrasonography has also been used to assess the status of the fetal cardiovascular system.[25] Referral of such patients to centers where better facilities for delivery and immediate postnatal therapy are available has resulted in considerable improvement in the prognosis of infants born with this condition.
The role of imaging in a patient referred for endovascular therapy is to non-invasively
demonstrate the number and site of arteriovenous fistulae, presence of thrombosis,
sinus abnormalities and venous drainage patterns. This is of particular importance
in neonates with VOGMs as the cardiac and other associated co-morbid conditions
limit the acceptable contrast load during angiography. Obtaining as much information
as possible from noninvasive imaging studies enables planning of diagnostic
angiography and intervention in the same sitting. This eliminates the risk
of repeated angiographic studies under anesthesia in such patients.[4],[26],[27],[34]
The multiplanar imaging capabilities of MRI, its high intrinsic tissue contrast
and its sensitivity to flow make it the modality of choice in the investigation
of patients referred for endovascular therapy. Infants who have been subjected
to interventional therapy can be followed up using neurosonography, while
transcranial Doppler and CT or MRI can be used in the older children and
adults.
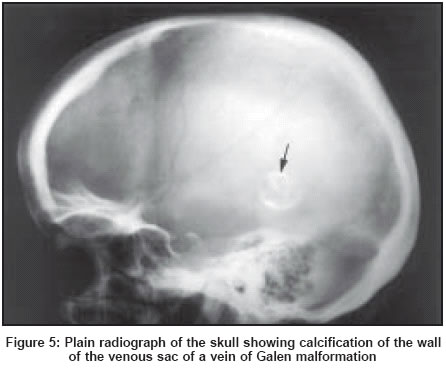
Radiography
Plain radiography of the skull contributes little to the diagnosis of VOGMs beyond the demonstration of a rim of calcification within the wall of the aneurysmal sac [Figure
- 5]. Calcification is seen in about half the patients with thrombosed VOGMS; compared to only 14% of patients without thrombosis.[27] Chest radiographs may reveal features of congestive heart failure such as cardiomegaly, widening of the superior mediastinum and retrosternal fullness. Retropharyngeal soft tissue prominence may be seen due to dilatation of the great vessels of the neck.[28]
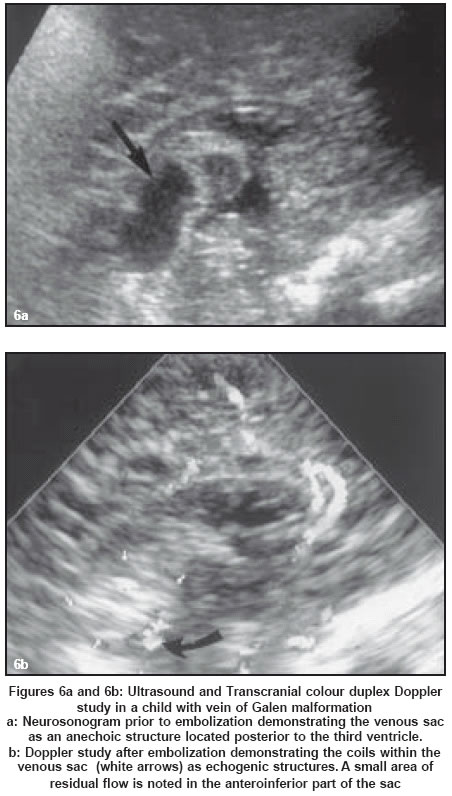
Ultrasound
Antenatal ultrasound scans demonstrate the venous sac as a sonolucent mass located posterior to the third ventricle. Ultrasonic demonstration of pulsatile flow within it helps in differentiating VOGMs from other midline cystic lesions. Associated venous anomalies can often be visualized. Evidence of hydrocephalus and cardiac dysfunction can also be obtained on antenatal ultrasonography.[21],[22],[23],[24],[25],[29]
In the postnatal period, Doppler ultrasonography can be used to demonstrate the hemodynamic changes associated with the malformation.[30] Ultrasound is of special significance in the follow-up of patients who have been treated with endovascular therapy [Figure
- 6], where progressive thrombosis of the venous sac can be demonstrated and the status of the shunt can be assessed on serial studies.[31],[32]
Computed tomography (CT)
Contrast enhanced axial CT scan of the brain usually demonstrates a well-defined, multilobulated, intensely enhancing lesion, located within the cistern of velum interpositum. Dilatation of the ventricular system, periventricular white matter hypodensities, as well as diffuse cerebral atrophy are the commonly associated findings.
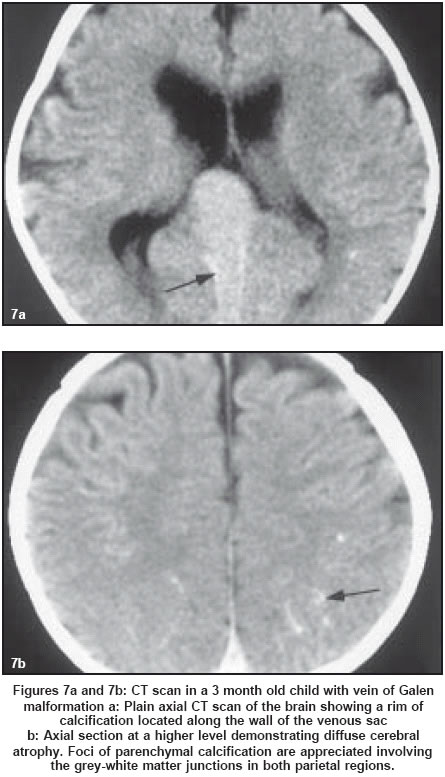
Features of cerebral parenchymal damage in the form of diffuse chronic ischemic
changes, parenchymal calcifications, generalized cerebral atrophy and focal
parenchymal infarcts are also demonstrated well on CT [Figure:7a].[4],[14] Jayakumar
et al described the de-novo development of cerebral parenchymal calcifications
in a child with VOGM, in whom ventriculoperitoneal shunt placement was performed
for hydrocephalus.[33]
The presence of thrombosis within the aneurysmal sac can be demonstrated well
on CT. Since the original description by Heinz et al in 1968, several reports
of spontaneous thrombosis of VOGMs have appeared in medical literature.[35],[27],[36],[37],[38] The
thrombus within the aneurysmal sac commonly appears as mixed hypodense, isodense
and hyperdense areas due to variable maturation of the clot. On contrast enhanced
CT, the presence of a central thrombus and peripheral circulating blood along
the wall of the sac can produce the so-called ′Target sign′.[27] The
dilatation of collateral parenchymal veins can usually be appreciated.
A crescentic rim of calcification is more commonly seen in patients with
thrombosed VOGMs [Figure:7b]. However, the presence of calcification has proved
to be
a poor predictor of the tendency of the lesion to subsequently thrombose.
Calcification is rarely seen before the age of 15 years and complete calcification
of the
sac is extremely rare.[39]
Magnetic resonance imaging (MRI)
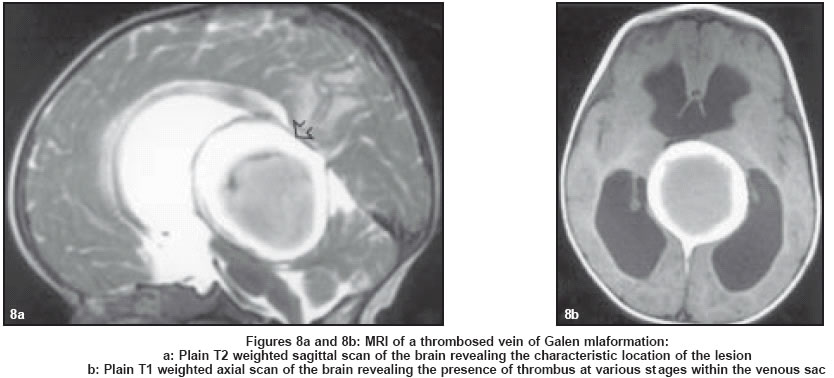
MRI is gaining popularity as the modality of choice for initial assessment of VOGMs. It can demonstrate the location of fistula, presence of any nidus, the arterial components, the venous sac as well as the status of venous drainage. Thrombosis of the venous sac is also depicted well on MRI [Figure
- 8]. The position and identity of major arterial trunks, primary branches as well as secondary branches feeding the fistula are better identified on MRI than on CT. Accurate identification of draining veins, venous anomalies and venous constraints is also possible with MRI. The exquisite soft tissue contrast of MRI makes it the modality of choice in the evaluation of the ventricular system and cerebral parenchymal changes. MR angiography is being increasingly used as a noninvasive alternative to diagnostic angiographic studies in the initial evaluation of these lesions.[26],[34]
Angiography
Angiography remains the gold standard for the evaluation of VOGMs. It scores over noninvasive modalities such as CT angiography and MR angiography in demonstrating small feeders supplying the fistula, as well as the dynamic aspects of the venous drainage of the normal brain, and hemodynamic relationships with the venous drainage of the arteriovenous shunt.[26],[34]
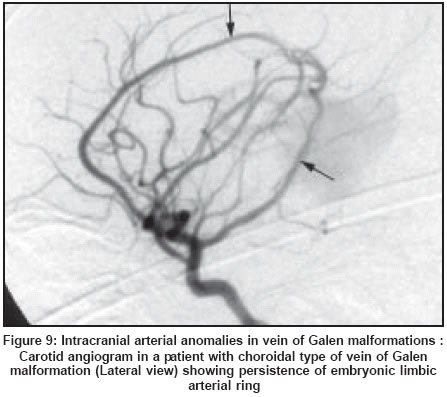
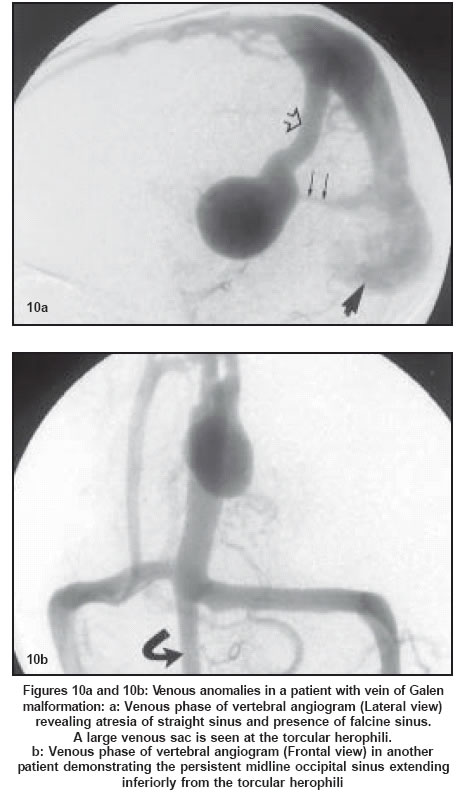
VOGMs are associated with several arterial and venous anomalies. These anomalies represent the persistence of embryological vascular patterns. The limbic ring represents a persistent arterial bridge between the anterior cerebral and anterior choroidal artery [Figure
- 9]. The absence or interruption of the straight sinus is a common association with these anomalies. Persistence of venous channels such as the falcine sinus, occipital sinus and marginal sinus may also be seen. Atresia of transverse and sigmoid sinuses may also be associated [Figure
- 10].
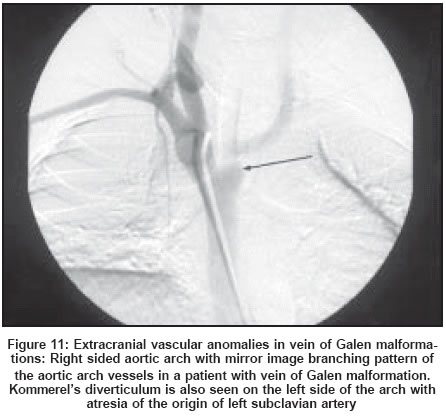
VOGMs are also associated with the Turner syndrome and blue rubber bleb
syndrome. Supernumerary digits, hypospadias, transposition of great vessels,
aortic stenosis and right-sided aortic arch have been reported in association
with VOGMs [Figure - 11].[34],[40],[41]
Management Untreated VOGMs have a very poor prognosis.[5],[14],[42],[43] A high proportion of patients who present in the neonatal period rapidly deteriorate and succumb to congestive cardiac failure. Rapid and aggressive management of the cardiac failure is essential. Aggressive medical management can usually postpone the intervention until the child is aged about 5 - 6 months, at which point intervention is easier and safer. Emergency embolization of the malformation may be necessary to reduce the shunt in neonates with congestive cardiac failure that is refractory to medical therapy.[4],[12],[43]
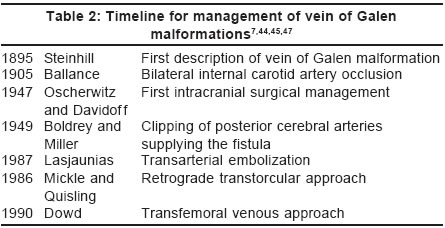
The evolution of the management of VOGMs over time is summarized in [Table
- 2].
Surgery
Considering the many problems associated with the management, these lesions have been termed as the ′Gordian knot′ of cerebrovascular surgery. Despite technological advances in microneurosurgery, complete elimination of the lesion by surgery is rarely achieved. The problems of major cranial surgery involving a deep-seated, high-flow shunt in an infant with multiorgan failure are compounded by the poor myelination of the brain parenchyma, which tends to tear easily on retraction.[34] Similarly, ventricular shunting may worsen the cerebral venous hypertension, and should be avoided before elimination of the arteriovenous shunt. This procedure is not tolerated by infants and must be preceded by emergency embolization.[12],[14] Endovascular management
Advances in the field of interventional neuroradiology have ensured significant improvements in outcome in these patients. Several studies have documented the efficacy and safety of endovascular treatment in these patients.[46],[47],[48],[49],[50],[51],[52] The timing of endovascular management is determined by the clinical presentation. Congestive cardiac failure in a neonate that is refractory to medical treatment is an indication for emergency embolization. The goal of therapy in such patients would be to arrest the congestive cardiac failure rather than to achieve complete obliteration of the shunt. In such children, it may be acceptable to perform partial embolization to reduce the arteriovenous shunt and facilitate normal systemic and neurological development, even with the presence of a residual shunt. The procedure can be performed in a staged manner to minimize complications. In a child who has not presented with cardiac failure, the aim of endovascular therapy would be to prevent consequences of chronic cerebral venous hypertension and to promote normal cerebral development.[4],[53] Treatment at the age of 5 months balances the benefits of safe embolization against the risk of cerebral damage. Imaging evidence of encephalomalacia is thus considered a relative contraindication to endovascular therapy.[11],[46]
Lasjaunias and co-workers, who have the largest experience in managing
these lesions, have discussed therapeutic decisions, based on the clinical
expression in the neonatal period. They described a 21-point scale based
on cardiac function, cerebral function, hepatic function, respiratory function
and renal function. A score of less than 8 usually indicates a poor prognosis
and does not warrant emergency management. A score of 8-12 is an indication
for emergency endovascular management. A score of > 12 indicates a well-preserved
neonate and attempts are made to delay the endovascular procedure, by medical
management. The presence of failure to thrive, unstable cardiac failure
or macrocrania are indications to advance the embolization.[54]
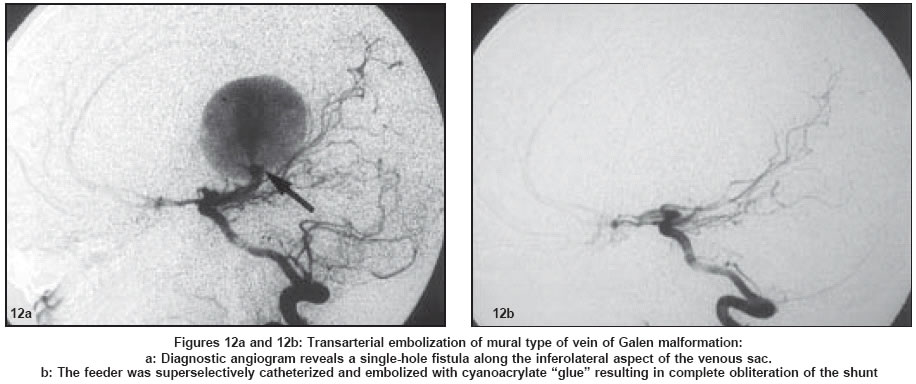
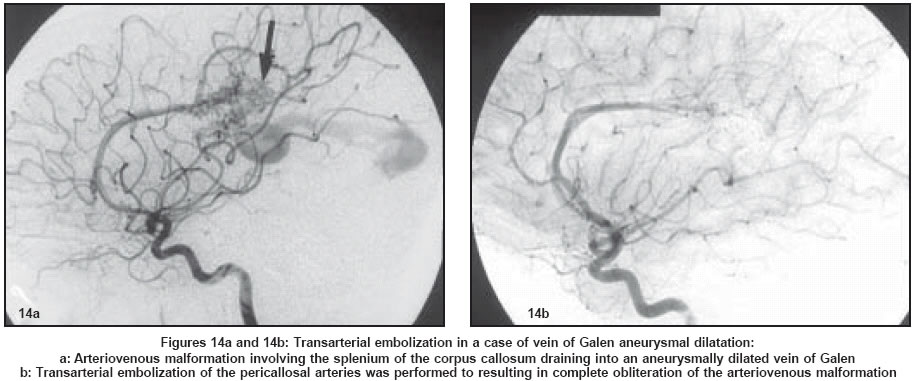
The choice of the specific endovascular approach depends on the angioarchitecture of the malformation. Arteriovenous fistulas are occluded on the arterial side, using embolic agents such as coils, cyanoacrylates and detachable balloons [Figure
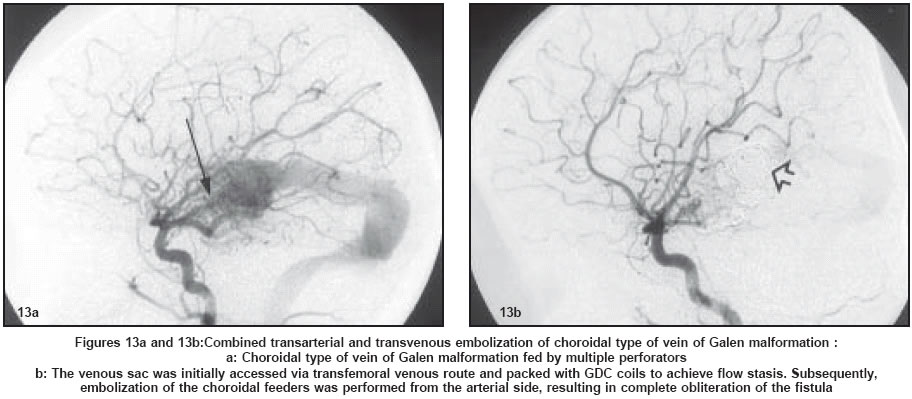
- 12]. This route is preferred for embolization by most authors. Transvenous and transtorcular coil embolization of the venous sac have been used to achieve flow reduction in selected cases with high-flow fistulas. Transvenous embolization has been described as the technique of choice in patients with multiple fistulas, as it results in retrograde thrombosis and obliterates the fistulas [Figure
- 13]. However, Lasjaunias and co-workers have recommended that venous embolization be reserved for patients in whom arterial route embolization is impossible or unsuccessful.[14] Venous embolization is also avoided in patients with parenchymal or choroidal arteriovenous malformations. These lesions are embolized from the arterial side to avoid venous hypertension [Figure
- 14].[46]
Complications
Potentially fatal complications of endovascular management include normal perfusion pressure breakthrough and intracerebral hemorrhage due to venous hypertension.[55] These can be largely avoided by staging the embolization procedure. Perforation of the venous sac has been reported to occur during positioning of the microcatheter during coil embolization, and can usually be managed by reversal of anticoagulation and continuation of coil embolization. Ischemic neurological deficits can occasionally be encountered after embolization. Pulmonary embolization with embolic agents is common considering the high flow across the intracranial shunt.
Conclusion Thus, with advances in imaging technology, cardiac care, developments in the field of interventional neuroradiology and availability of better post-procedure intensive care, these once non-treatable conditions with a very high mortality rate, are now potentially curable using interventional neuroradiological techniques, with excellent clinical results, low complication rate and very low morbidity and mortality. In the future, with the establishment of more and more centers with such facilities in the country, the treatment of this condition will be within the reach of all patients.
References
| 1. | Casasco A, Lylyk P, Hodes JE, Kohan G, Aymard A, Merland JJ. Percutaneous transvenous catheterization and embolization of vein of Galen aneurysms. Neurosurgery 1991;28:260-6. Back to cited text no. 1 |
| 2. | Ciricillo SF, Edwards MS, Schmidt KG, Hieshima GB, Silverman NH, Higashida RT, et al. Interventional neuroradiological management of vein of Galen malformations in the neonate. Neurosurgery 1990;27:22-8. Back to cited text no. 2 |
| 3. | Raybaud CA, Strother CM, Hald JK. Aneurysms of the vein of Galen: embryonic considerations and anatomical features relating to the pathogenesis of the malformation. Neuroradiology 1989;31:109-28. Back to cited text no. 3 [PUBMED] |
| 4. | Berenstein A, Lasjaunias P. Arteriovenous fistulas of the brain. In: Surgical Neuroangiography 4. Endovascular treatment of cerebral lesions. Berlin: Springer-Verlag; 1992. pp. 267-317. Back to cited text no. 4 |
| 5. | Yasargil MG. Microneurosurgery IIIB. New York: Thieme Medical Publishers; 1988. pp. 323-57. Back to cited text no. 5 |
| 6. | Garcia-Monaco R, Lasjaunias P, Berenstein A. Therapeutic management of vein of Galen aneurysmal malformations. In: Vinuela F, Halbach VV, Dion JE, editor. Interventional Neuroradiology: Endovascular therapy of the central nervous system. New York: Raven Press; 1992. pp. 113-27. Back to cited text no. 6 |
| 7. | Lasjaunias P, Terbrugge K, Piske R, Lopez Ibor L, Manelfe C. Vein of Galen dilatation: Anatomo-clinical forms and endovascular treatment. Fourteen cases explored and / or treated between 1983 and 1986. Neurochirugie 1987;33:315-33. Back to cited text no. 7 [PUBMED] |
| 8. | Hoffman HJ. Malformations of the Vein of Galen. In: Edwards MSB, Hoffmann HJ, eds. Current Neurosurgical Practice: Cerebral vascular disease in children and adolescents. Baltimore: Williams and Wilkins; 1989. pp. 239-46. Back to cited text no. 8 |
| 9. | Crawford JM, Rossitch E Jr, Oakes WJ, Alexander E 3rd. Arteriovenous malformation of the great vein of Galen associated with patent ductus arteriosus. Childs Nerv Syst 1990;6:18-22. Back to cited text no. 9 [PUBMED] |
| 10. | Pellegrino PA, Milanesi O, Saia OS, Carollo C. Congestive heart failure secondary to cerebral arterio-venous fistula. Childs Nerv Syst 1987;3:141-4. Back to cited text no. 10 |
| 11. | Bhattacharya JJ, Thammaroj J. Vein of Galen Malformations. J Neurol Neurosurg Psychiatr 2003;74:142-4 Back to cited text no. 11 |
| 12. | Zerah M, Garcia-Monaco, Rodesh G, Terbrugge K, Tardieu M, de Victor D, et al. Hydrodynamics in vein of Galen malformations. Childs Nerv Syst 1992;8:111-7. Back to cited text no. 12 |
| 13. | Sainte-Rose C, La Combe J, Pierre-Kahn A, Renier D, Hirsch JF. Intracranial venous sinus hypertension: Cause or consequence of hydrocephalus in infants? J Neurosurg 1984;60:727-36. Back to cited text no. 13 |
| 14. | Lasjaunias P, Garcia-Monaco R, Rodesch G, Ter Brugge K, Zerah M, Tardieu M, et al. Vein of Galen malformation: Endovascular management of 43 cases. Childs Nerv Syst 1991;7:360-7. Back to cited text no. 14 |
| 15. | Gulati S, Kalra V. An Uncommon Variety of Vein of Galen Malformation. Indian Pediatr 2002;39:307-8. Back to cited text no. 15 [PUBMED] [FULLTEXT] |
| 16. | Gold AP, Ransohoff JR, Carter S. Vein of Galen malformation. Acta Neurol Scand 1964;40:5-7. Back to cited text no. 16 |
| 17. | Kothari SS, Naik N, Juneja R, Saxena A. Aneurysm of Vein of Galen in the neonates: Report of four cases. Indian Heart J 2001;53:499-502. Back to cited text no. 17 |
| 18. | Cumming GR. Circulation in neonates with intracranial arteriovenous fistula and cardiac failure. Am J Cardiol 1980;45:1019-24. Back to cited text no. 18 |
| 19. | Garcia-Monaco R, de Victor D, Mann C, Hannedouche A, Terbrugge K, Lasjaunias P. Congestive cardiac manifestations from cerebrocranial arteriovenous shunts: Endovascular management in 30 children. Childs Nerv Syst 1991;7:48-52. Back to cited text no. 19 |
| 20. | Lasjaunias P, Terbrugge K, Lopez Ibor L, Chiu M, Flodmark O, Chuang S, et al. The role of dural venous anomalies in vein of Galen aneurysms: report of six cases and review of the literature. AJNR Am J Neuroradiol 1987;8:185-92. Back to cited text no. 20 |
| 21. | Vintzileos AM, Eisenfeld LI, Campbell WA, Herson VC, DiLeo PE, Chameides L. Prenatal ultrasonic diagnosis of arteriovenous malformation of the vein of Galen. Am J Perinatol 1986;3:209-11. Back to cited text no. 21 |
| 22. | Mendelson DB, Hertzanu Y, Butterworth A. In utero diagnosis of a vein of Galen aneurysm by ultrasound. Neuroradiology 1984;26:417-8. Back to cited text no. 22 |
| 23. | Reiter AA, Huhta JC, Carpenter RJ Jr, Segall GK, Hawkins EP. Prenatal diagnosis of arteriovenous malformation of the vein of Galen. JCU 1986;14:623-8. Back to cited text no. 23 |
| 24. | Hirsch JH, Cyr D, Eberhardt H, Zunkel D. Ultrasonographic diagnosis of an aneurysm of the vein of Galen in utero by duplex scanning. J Ultrasound Med 1983;2:231-3. Back to cited text no. 24 [PUBMED] |
| 25. | Jeanty P, Kepple D, Roussis P, Shah D. In utero detection of cardiac failure from an aneurysm of the vein of Galen. Am J Obstet Gynecol 1990;163:50-1. Back to cited text no. 25 |
| 26. | Seidenwurm D, Berenstein A, Hyman A. Vein of Galen malformation: Correlation of clinical presentation, arteriography and MR imaging. AJNR Am J Neuroradiol 1991;12:347-54. Back to cited text no. 26 |
| 27. | Nikas DC, Proctor MR, Scott RM. Spontaneous thrombosis of vein of Galen aneurysmal malformation. Paediatr Neurosurg 1999;31:33-9. Back to cited text no. 27 [PUBMED] [FULLTEXT] |
| 28. | Swischuk LE, Crowe JE, Mewborns EJ Jr. Large vein of Galen aneurysms in the neonate: a constellation of diagnostic chest and neck radiologic findings. Pediatr Radiol 1977;6:4-9. Back to cited text no. 28 |
| 29. | Chiang V, Awad I, Berenstein A, Scott M, Spetzler R, Alexander MJ. Galenic arteriovenous malformation. Neurosurgery 1999;44:847-54. Back to cited text no. 29 |
| 30. | Surana UM, Patel BN, Patel SB, Dhebar M. Images: Vein of Galen malformation. Ind J Radiol Imag 1999;9:21-2. Back to cited text no. 30 |
| 31. | Deeg KH, Scarf J. Colour Doppler imaging of arteriovenous malformation of the vein of Galen in a newborn. Neuroradiology 1990;32:60-3. Back to cited text no. 31 |
| 32. | Tessler FN, Dion J, Vinuela F, Perrella RR, Duckwiler G, Hall T, et al. Cranial arteriovenous malformations in neonates:colour Doppler imaging with angiographic correlation. AJR Am J Roentgenol 1989;153:1027-39. Back to cited text no. 32 |
| 33. | Jayakumar PN, Sathish Chandra P. Cerebral parenchymal calcification in a child with vein of Galen malformation - Role of medullary veins. Neurology India 1997;45:194-76. Back to cited text no. 33 |
| 34. | Horowitz MB, Jungreis CA, Quisling RG, Pollack I. Vein of Galen aneurysms: A review and current perspective. AJNR Am J Neuroradiol 1994;15:1486-96. Back to cited text no. 34 |
| 35. | Heinz ER, Schwartz JF, Sears RA. Thrombosis in the vein of Galen malformation. Br J Radiol 1968;41:424-8. Back to cited text no. 35 |
| 36. | Dean DF. Management of clotted aneurysm of the vein of Galen. Neurosurgery 1981;8:589-92. Back to cited text no. 36 |
| 37. | Whitaker JB, Latack JT, Venes JL. Spontaneous thrombosis of a vein of Galen aneurysm. AJNR Am J Neuroradiol 1987;8:1134-6. Back to cited text no. 37 |
| 38. | Six EG, Cowley AR, Kelly DL Jr, Laster DW. Thrombosed aneurysm of the vein of Galen. Neurosurgery 1980;7:274-8. Back to cited text no. 38 |
| 39. | Chapman S, Hockley AD. Calcification of an aneurysm of the vein of Galen. Pediatr Radiol 1989;19:541-2. Back to cited text no. 39 |
| 40. | Jarrell HR, Schochet SS Jr Krous H. Turner's syndrome and vein of Galen aneurysm: a previously unreported association. Acta Neuropathol 1981;55:189-91. Back to cited text no. 40 |
| 41. | Rosenblum WI, Nakoneczna I, Konderding HS. Multiple vascular malformation in the "blue rubber bleb nevus" syndrome: a case with aneurysm of vein of Galen and vascular lesions suggesting a link of the Weber-Osler-Rendu syndrome. Histopathology 1978;2:301-11. Back to cited text no. 41 |
| 42. | Johnston IH, Whittle IR, Besser M, Morgan MK. Vein of Galen malformation: Diagnosis and management. Neurosurgery 1987;20:747-58. Back to cited text no. 42 |
| 43. | Hoffmann HJ, Chuang S, Hendrick EB, Humphreys RP. Aneurysms of the vein of Galen: Experience at the Hospital for Sick Children, Toronto. J Neurosurg 1982;57:316-22. Back to cited text no. 43 |
| 44. | Hamilton MG, Herman JM, Khayata MH, Spetzler RF. Aneurysms of the vein of Galen. In. Youmans JR, ed. Neurological Surgery. 4th edn. Philadelphia: WB Saunders Company; 1996. pp. 1491 - 510. Back to cited text no. 44 |
| 45. | Mickle JP, Quisling RG. The transtorcular embolization of vein of Galen aneurysms. J Neurosurg 1986;64:731-5. Back to cited text no. 45 |
| 46. | Lasjaunias P, Rodesch G, Terbrugge K, Pruvost P, Devictor D, Comoy J, et al. Vein of Galen aneurysmal malformations: report of 36 cases managed between 1982 and 1988. Acta Neurochir 1989;99:26-37. Back to cited text no. 46 |
| 47. | Dowd CF, Halbach W, Barnwell SL, Higashida RT, Edwards MS, Hieshima GB. Transfemoral venous embolization of vein of Galen malformations. AJNR Am J Neuroradiol 1990;11:643-8. Back to cited text no. 47 |
| 48. | Casasco A, Lylyk P, Hodes JE, Kohan G, Aymard A, Merland JJ. Percutaneous transvenous catheterization and embolization of vein of Galen aneurysms. Neurosurgery 1991;28:260-5. Back to cited text no. 48 |
| 49. | Mickle AP. The transtorcular embolization of vein of Galen aneurysms and update on the use of this technique in twenty four patients. In: Marlin AE, ed. Concepts in Pediatric Neurosurgery. Basel: Karger 1991;11:69-78. Back to cited text no. 49 |
| 50. | Lylyk P, Vineula F, Dion JE, Duckwiler G, Guglielmi G, Peacock W, et al. Therapeutic alternatives for vein of Galen vascular malformation. J Neurosurg 1993;78:438-45. Back to cited text no. 50 |
| 51. | Halbach VV, Dowd CF, Higashida RT, Balousek PA, Ciricillo SF, Edwards MS. Endovascular treatment of mural type vein of Galen malformations. J Neurosurg 1998;89:74-80. Back to cited text no. 51 |
| 52. | Mitchell PJ, Rosenfield JV, Dargaville P. Endovascular management of vein of Galen aneurysmal malformations presenting in the neonatal period. AJNR Am J Neuroradiol 2001;22:1403-9. Back to cited text no. 52 |
| 53. | ter Brugge KG. Vein of Galen management in neonatal period. Am J Neuroradiol 2001;22:1403-9. Back to cited text no. 53 |
| 54. | Lasjaunias P, Alvarez H, Rodesch G, Garcia-Monaco R, Terbrugge K, Burrows P, et al. Aneurysmal malformations of the vein of Galen. Follow up of 120 children treated between 1984 and 1994. Interventional Neuroradiology 1996;2:15-26. Back to cited text no. 54 |
| 55. | Spezler RF, Wilson CB, Weinstein P. Normal perfusion pressure breakthrough theory. Clin Neurosurg 1978;25:651-72. Back to cited text no. 55 [PUBMED] [FULLTEXT] |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04012f13.jpg]
[ni04012f7.jpg]
[ni04012f1a.jpg]
[ni04012t1.jpg]
[ni04012f14.jpg]
[ni04012t2.jpg]
[ni04012f4.jpg]
[ni04012f1b.jpg]
[ni04012f9.jpg]
[ni04012f6.jpg]
[ni04012f10.jpg]
[ni04012f2.jpg]
[ni04012f3.jpg]
[ni04012f8.jpg]
[ni04012f12.jpg]
[ni04012f11.jpg]
[ni04012f5.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}