 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
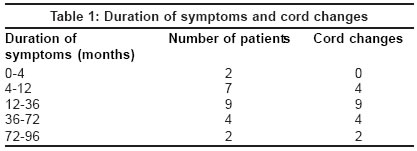
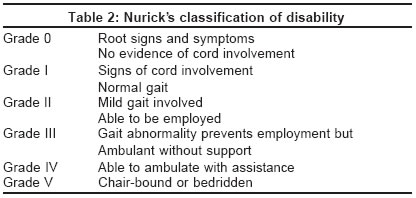
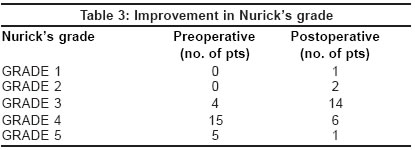
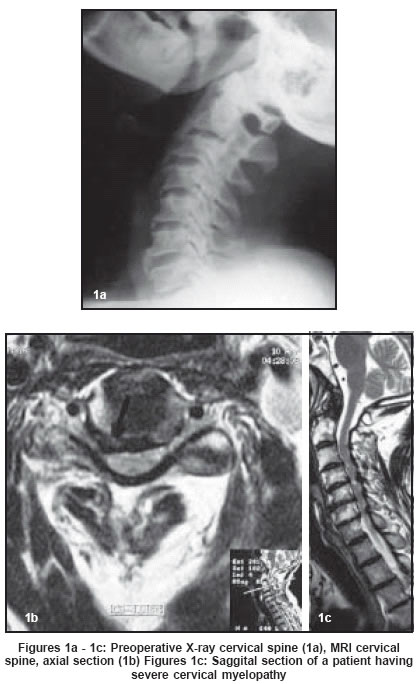
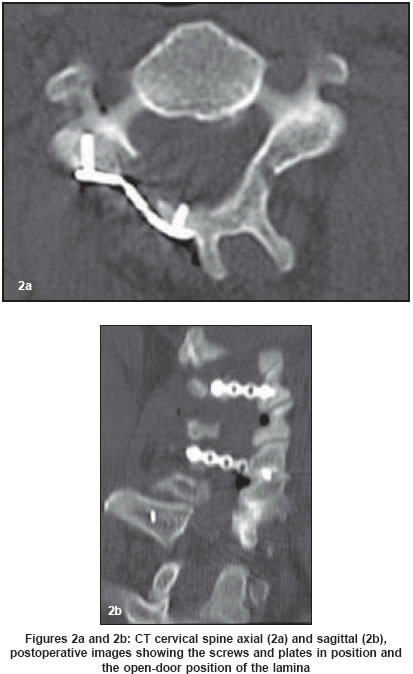
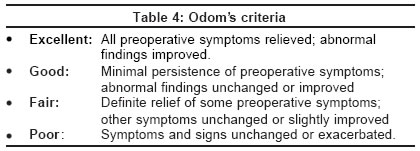
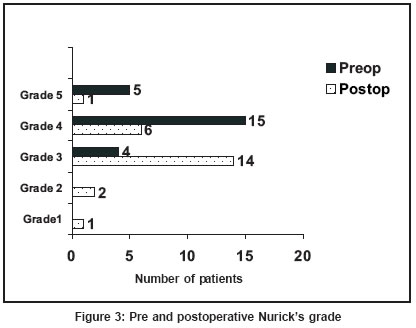
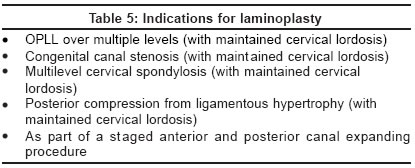
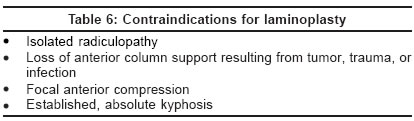
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 54-58 Original Article Efficacy and results of expansive laminoplasty in patients with severe cervical myelopathy due to cervical canal stenosis Agrawal D, Sharma BS, Gupta A, Mehta VS Department of Neurosurgery, Neurosciences center, All India Institute of Medical Sciences,New Delhi - 110029 Code Number: ni04013 Abstract Aims and objectives: To assess the efficacy and results of expansive laminoplasty in advanced (Nurick’s Grade III or greater) cervical myelopathy. Materials and Methods: We reviewed data in 24 patients who underwent cervical laminoplasty from January 1999 to December 2002. Nuricks grading was used for quantifying the neurological deficits and outcome analysis was done using Odom’s criteria. A modified Hirabayashi’s open door laminoplasty was done using Titanium miniplates and screws in 22 patients, autologous bone in one and hydroxyapatite spacer in one patient. Observations: There were 3 females and 21 males with a mean age of 56 years (range 39-72 years). Four patients presented in Nuricks Grade III, 15 in Grade IV and five in Grade V. MR imaging showed MSCS in 21 cases, OPLL in nine cases and ligamentum flavum hypertrophy in nine cases with cord signal changes being present in 19 cases. Results: All patients with duration of symptoms less than three years, and 50 % with duration ranging from three to six years had improvement by at least one Nurick’s grade following surgery. Eighty-seven per cent Grade IV patients (ambulatory with support) improved to Grade III (ambulatory without support) following laminoplasty. Using Odom’s criteria, 23 patients (95.8%) had a good to fair outcome. Conclusions: Cord decompression with expansive laminoplasty using titanium miniplate fixation may improve the neurological outcome even in patients presenting late, and improvement by even one grade may have major ‘quality of life’ benefits for these patients. Introduction Cervical canal stenosis is caused by the narrowing of the central spinal canal or neural foramina and may be either developmental in origin, or secondary to bony and/or soft tissue changes caused by multisegmental cervical spondylosis (MSCS) or ossification of the posterior longitudinal ligament (OPLL). Cervical laminectomy and laminoplasty have been used to decompress the neural elements posteriorly when there is extensive involvement of the cervical spine.[1] Laminoplasty, which preserves the posterior elements, is considered the preferred posterior procedure.[2],[3],[4],[5],[6] However, there have been no large series with patients having clinically advanced disease. We analyze our experience with this procedure in patients with symptoms of severe cervical myelopathy, done over a four-year period. Materials and methods In this retrospective study, all patients who were admitted and underwent laminoplasty in the department of neurosurgery, from January 1999 through December 2002 (four-year period) were included. The demographic and clinical details, radiological investigations, operation details at admission and at follow-up were analyzed.Operative technique Observations Demographic profile Clinical features Radiology Operating time Complications CSF leak occurred in one patient, which resolved on conservative management. There was no mortality in this series. Follow-up Results Three patients in Nurick′s Grade III improved to either Nurick′s Grade I (n=1) or Nurick′s Grade II (n=2) following the laminoplasty. Thirteen out of the 15 patients (86.6%) who were in Grade IV (ambulatory with support) improved to Nurick′s Grade III (ambulatory without support) postoperatively. Surprisingly, four of the five patients (80%) in Nurick′s Grade V had improved to Grade IV following the laminoplasty, at last follow-up. Outcome assessment was done using Odom′s criteria [Table - 4] and using these criteria, 23 patients (95.8%) had a good to fair outcome. All patients with duration of symptoms less than three years, and 50 % of the patients with duration of symptoms ranging from three to six years had improvement by at least one Nurick′s grade following surgery [Figure - 3]. However, patients with duration of symptoms more than six years did not show any improvement in Nurick′s grade following surgery. Patients who had cord signal changes on both T1 and T2 weighted images on MRI had a poorer prognosis compared to patients who had cord signal changes only on T2 weighted images. Patients having cord signal changes only on T2 weighted images improved by at least one Nurick′s grade, compared to patients having cord signal changes on both T1 and T2 weighted images, who did not show any improvement in Nurick′s grade following the laminoplasty. Discussion Anterior and posterior decompression are established techniques in the management of multilevel cervical canal stenosis resulting in myeloradiculopathy.[9],[10],[11],[12] In the past, laminectomy had been the most common method to achieve posterior decompression of the cervical spine in these patients. However, the procedure was complicated by postoperative instability resulting in deformity, particularly kyphosis,[9],[11],[12] as well as postoperative laminectomy membrane formation resulting in restenosis and arachnoiditis.[3] Anterior cervical decompression with spinal fusion is also practiced widely in patients with cervical spondylotic myeloradiculopathy.[13] However, a consequence of this procedure is the immobilization of multiple segments, which has been shown to lead to long-term changes at adjacent vertebral levels.[14] Laminoplasty was developed to avoid these complications, with the first expansive open door laminoplasty being described by Hirabayashi et al,[3] and which since than has been further modified by Hirabayashi and others.[7],[15] The elegance of this procedure lies in its simplicity with results comparable to laminectomy and anterior decompression. Itoh and Tsuji,[7] besides others, have shown increased stability, with less sliding, tilting, and range of motion after laminoplasty compared with laminectomy. This may be protective against postoperative instability. Various modifications have been advised by various authors to maintain the ′open′ book position of the posterior elements during laminoplasty. These are often complicated, requiring tedious wiring and bone-grafting techniques that increase the operative time, blood loss, donor site pain and infection, besides increasing the technical difficulty. These considerations could easily outweigh the possible benefits of laminoplasty over laminectomy. Titanium miniplate fixation, originally performed by O′Brien, offers all the advantages of laminoplasty without its drawbacks and offers a simple, durable and efficient technique to maintain the postoperative position of the open door.[7] However, specific indications and contraindications for performing laminoplasty [Table - 5] and [Table - 6] have been described and patient selection remains important for the success of the procedure.[6] Long-term results are also now available on laminoplasty. Iwasaki M, [4] studied 64 patients with OPLL who underwent expansive laminoplasty for more than 10 years (mean follow-up 12.2 years) and found that the neurological recovery was maintained in 60% of the patients. Kyphosis was present in 8% of the patients, although it was not found to be associated with neurological deterioration. The authors recommended expansive and extensive laminoplasty for OPLL. Inoue H,[5] studied long-term outcome (greater than 5 years) in patients with myelopathy due to cervical spondylosis and OPLL who underwent expansive laminoplasty, and complete decompression was maintained in 84% of the patients with myelopathy due to cervical spondylosis. The average follow-up in our series was 22 months, which is relatively short to give long-term results. However, as all patients in our study had an advanced disease at presentation, the results are significant. Postoperative improvement was also maintained in all our patients at the last follow-up. Quantification of deficits for assessing the results of the spinal surgery is also important and Nurick, in 1972, devised a classification for cervical spondylotic myelopathy, largely based on gait disturbances [Table - 2].[16] The overwhelming appeal of this classification lies in its simplicity and that it can be applied easily to retrospective data. For this reason Nurick′s classification was chosen for the quantification of deficits in this study. However, as it is based mainly on gait abnormalities, sensory deficits as well as bladder dysfunction are not considered and remain important limitations. Though the JOA scale overcomes these limitations, it is more complex and cannot be applied easily to retrospective data.[17] For outcome analysis we used the Odom′s scale,[18] as it is the most commonly used scale and is relatively simple [Table - 4]. Using Odom′s criteria, 23 patients (95.8%) had good to fair outcome (improvement by at least one grade) in the immediate postoperative period and the improvement was continuing or sustained at the last follow-up. More importantly, 13 out of 15 patients (86.6%) who were in Grade IV (ambulatory with support) became ambulatory without support (Grade III). This shows that improvement by even one grade may have major ′quality of life benefits′ for these patients. Another interesting finding of our study was the postoperative improvement by at least one Nurick′s grade in 50 % percent of the patients with duration of symptoms between three and six years. This implies that the disease process may be partially reversible, even in patients presenting late, though early surgery carries the best prognosis. Our study assumes significance in view of the fact that the majority (80%) of the patients were in Nurick′s Grade IV or V, implying having advanced disease. Laminoplasty was found to be especially beneficial in these patients as almost all showed neurological improvement with minimal morbidity and no mortality. Conclusion This is one of the largest studies on patients presenting with severe cervical myelopathy and shows that cord decompression using expansive laminoplasty using titanium miniplate fixation may improve the neurological outcome even in patients presenting late, and improvement by even one grade may have major ′quality of life benefits′ for these patients. Expansive laminoplasty using titanium miniplate fixation offers all the advantages of laminectomy without its drawbacks and offers a simple, durable and efficient technique to maintain the postoperative open-door position , especially in patients with advanced disease. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04013t3.jpg] [ni04013f3.jpg] [ni04013t2.jpg] [ni04013t6.jpg] [ni04013t5.jpg] [ni04013t1.jpg] [ni04013f2.jpg] [ni04013t4.jpg] [ni04013f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}