 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
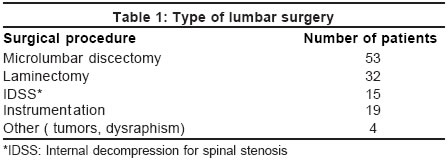
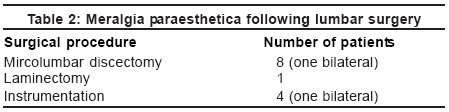
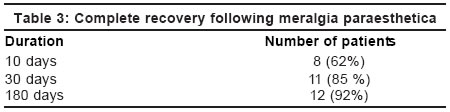
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 64-66 Original Article Meralgia paraesthetica following lumbar spine surgery: A study in 110 consecutive surgically treated cases Gupta A, Muzumdar D, Ramani PS Lilavati Hospital and Research Centre and Shushrusha Citizens Co-operative Hospital, Mumbai Code Number: ni04015 Abstract Background: Lateral cutaneous femoral nerve (LCFN) injury or Meralgia paraesthetica (MP) results in restriction of activity. Compression of the nerve by disc hernia, retroperitoneal tumors, and external pressure around the anterior superior iliac spine is common. However, it is not commonly observed after lumbar spinal surgery in prone position. Study design: In this prospective study of 110 patients who underwent elective lumbar spinal surgery, managed from January 2002 to June 2002, the incidence, possible risk factors, etiopathogenesis and management of MP were analyzed. Results: There were 66 males and 44 females. The age of the patients ranged from 15 to 81 years (mean 46.9 yrs.). Thirteen patients (12%) suffered from MP. It is more common in thinner individuals due to pressure injury to the nerve at its exit point. Ninety-two per cent of the patients were asymptomatic at follow-up after 6 months. In 7 out of 13 patients, patchy sensory loss on clinical examination was seen at 6 months. Conclusion: MP after posterior lumbar spinal surgery is uncommon. Smaller bolsters may avoid some of the vulnerable pressure points, as the surface area available is relatively smaller. The posts of the Hall-Relton frame over the anterior superior iliac crest should be adequately padded. The condition is usually self-limiting. Surgical division or decompression of the LCFN is reserved for persistent or severe MP.Introduction Meralgia paraesthetica (MP) is a clinical syndrome resulting from the entrapment of the lateral femoral cutaneous nerve (LFCN) of the thigh in the inguinal region.[1],[2],[3] It is characterized as being disagreeably numb or a burning, tingling or pricking sensation over the anterolateral aspect of one or rarely both thighs. It is commonly observed following chronic irritation of the nerve due to mechanical factors exerting a downward pull or traction on the inguinal ligament. Obesity, pulmonary obstructive disease with a chronic cough and anatomical variations in the course of the nerve are common predisposing factors. The occurrence of MP following lumbar spine surgery is uncommon and there are few reports in the literature on this subject.[4] A prospective study analyzing the incidence, etiopathogenesis and management of this condition is discussed and the relevant literature is briefly reviewed. Material and Methods One hundred and ten patients of lumbosacral spine degenerative disease including high and low lumbar levels underwent surgery in the prone position over a period of six months from January 2002 to June 2002. Preoperative neurological assessment was carried out with special attention to the sensory, motor system and the reflexes. The surgeries mainly included microlumbar discectomy, laminectomy, internal decompression for spinal stenosis, and posterior lumbar interbody fusion [Table - 1]. Microlumbar surgery was carried out through a small paramedian incision on one side of the spine. All the other procedures were carried out through midline incision. The operation time ranged from 90-500 minutes. Blood loss during surgery ranged from 100-400 ml. Clinical examination showed partial or dense sensory loss along the distribution of the lateral cutaneous nerve of the thigh on the anterolateral aspect of the thigh [Figure - 1]. Local anesthesia was not administered to produce relief of pain or paraesthesias and confirm the diagnosis of MP. Neurophysiological examination including sensory nerve conduction or dermatome somatosensory evoked potentials was also not performed. Results There were 66 males and 44 females. The age of the patients ranged from 15 to 81 years (mean 46.9 yrs.). The weight of the patients ranged from 42 to 110 kg (mean 66.7 kg). Nineteen patients (11 males and 8 females) suffered from diabetes mellitus and 32 patients suffered from hypertension (14 males and 18 females). Hypertension and diabetes mellitus were common in 14 patients (6 males and 8 females). All patients were assessed at follow-up after 1-6 months. The mean follow-up duration was 4 months. Thirteen patients complained of MP, 11 patients on one side and 2 patients on both sides. The patients mentioned about an unpleasant feeling in the same evening of the day of the operation or on the next day in the morning. The feelings were of two types: 9 patients complained of abnormal unpleasant paraesthesiae and 4 patients complained of numbness over the anterolateral aspect of the thigh [Table - 2]. Sixty-two per cent (62%) patients were relieved of MP in 10 days, 85% patients in 1 month and 92% patients were asymptomatic in 6 months duration [Table - 3]. In the 8 patients who underwent microlumbar disc surgery, one had bilateral dysesthesiae, 3 patients had symptoms on the same side as the disc prolapse and 4 patients on the opposite thigh. The ailment was seen more in younger patients than adults with an average age of 38.2 years as against the average age of 46.9 years in the series. Only 2 patients had hypertension and 1 patient had diabetes mellitus. It was more frequently seen in young thinner individuals (11 patients) than elderly obese patients (2 patients). The average weight of the thinner individuals developing MP was 45.2 kg in comparison to the average weight of 68.4 kg in those who did not develop MP. In 12 patients the abnormal feeling was seen within 12 hours and in 1 patient it was observed on the fourth day. The feeling was most intense on first day, became slightly less on the third day and on the tenth day 40% patients had totally improved and forgotten about the ailment. At 1 month, the abnormal feeling although present was not unpleasant in 3 patients and only 1 patient remembered the abnormal feeling at 6 months although sensory loss (patchy) in the distribution of the LCFN of the thigh was present in 7 patients. In 7 out of 13 patients, patchy sensory loss on clinical examination was seen at 6 months. Oral Gabapentin 300 mg thrice a day for 3 weeks was administered empirically although no randomized trial has been conducted to study its efficacy in MP. Discussion LCFN arises in the lumbar plexus from L2 and L3 nerve roots. It has a constant course in the iliac fossa. The nerve comes out piercing the Poupart′s ligament medial to the anterior superior iliac spine remaining superficial to the sartorius muscle but deeper to the deep fascia. About 4 inches below this point it becomes subcutaneous. However, the exit point varies significantly. Aszmann et al observed that in 5 of the 9 cadavers dissected, the exit of the nerve was more than 1 centimeter away from the anterior superior iliac spine.[5] In another study of 52 human specimens the nerve in 54% of the cases was found to be directly susceptible to pressure.[6] De Ridder et al found abnormal anatomy in 26% of cadavers.[7] The exit point of the nerve is most vulnerable and susceptible to compression and constitutes entrapment neuropathy.[5] Since MP is characterized by pure sensory symptoms, there is no muscle weakness produced by the entrapment of the nerve. It is frequently misdiagnosed and can be attributed to surgical sequelae. A rare occurrence observed by the senior author is the feeling of burning occurring several weeks after the surgery. It is diffuse and is not restricted to the distribution of the LFCN. Its late occurrence does not argue in favor of the entrapment of this nerve. An autonomic disturbance occurring following surgery is possible since it is relieved following a ganglion block. The common etiologies of LCFN entrapment include iliac crest bone graft harvesting and seat belt injury in a vehicular accident.[8],[9],[10] The exact significance of chronic medical disease, especially diabetes mellitus, and hypertension in the etiopathogenesis of MP is not clearly defined. The weight of the patient and the duration of the surgery may contribute proportionately towards the etiology or outcome of MP. In addition, it is highly probable that intraoperative hypotension and significant blood loss during surgery could make nerves more susceptible to compression. It is observed in both sexes and is more prevalent in thinner individuals suggesting the theory of direct compression of this delicate nerve in the prone position. The patient usually mentions about MP within hours of surgery or might observe it on the following morning after surgery. The symptoms can manifest even on the fifth day.[11] We preferred to administer Gabapentin in a small dose of 300 mg three times a day for 3 weeks to these patients although its efficacy in MP is controversial. However, the results were encouraging in patients at the time of discharge from the hospital. They were quite happy, comfortable and required minimal reassurance. MP is an expression of pressure neuropathy caused by pressure of the bolster on the nerve at its exit and occurring in people sleeping prone on a wooden surface.[6],[12] The pressure on the nerve causes injury to the nerve resulting in axonotmesis or neurotomesis.[11] The final presentation of either numbness or unpleasant paraesthesiae depends on the type of injury. It is reported to occur following frog leg position used in coronary bypass surgery.[13] Compression of the LCFN can mimic a high lumbar disc herniation.[14] We treated 7 patients with a high lumbar herniated disc, and none had signs and symptoms of MP. It can get involved in the extraperitoneal approach to the anterior spine during handling of the psoas muscle. The nerve lies anteriorly and then traverses posterolateral to the psoas to reach the iliacus muscle. It can be injured at the anterior border of psoas.[4] We approached the anterior border of psoas taking precaution to avoid damage the ascending lumbar vein, thus preventing MP. The harvesting of bone grafts from the iliac crest can damage this nerve [9],[10] and laparoscopic surgeons performing inguinal hernia repair must be aware of this problem.[15],[16] The incidence of MP in our series was 12%. There are few comparable series in the literature. However, Mirovsky in his series had 20% incidence after spinal surgery in prone position.[4] A much higher incidence in his series possibly relates to the Hall-Relton frame used by him instead of bolsters. Our bolsters are standard, 26 inches long and 13 inches in circumference. Smaller bolsters may avoid some of the vulnerable pressure points, as the surface area available is relatively smaller. The posts of the Hall-Relton frame over the anterior superior iliac crest should be adequately padded. As the LCFN of the thigh is sensory, it produces only discomfort without any muscle weakness. It is usually self-limiting and does not require any specific treatment. In the past, small doses of chlorpromazine produced good results in these patients. Surgical division or decompression of the LCFN is reserved for patients having persistent or severe pain. Acknowledgements We are thankful to Dr. V. R. Bhimani, Executive Vice President and Shri Prakash V. Mhatre, Director, Operations of the Lilavati Hospital and Research Center and Dr. Mrs. A. Joshi, Dean, Shushrusha Cooperative Hospital for permission to do this study. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04015t2.jpg] [ni04015t3.jpg] [ni04015t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}