 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
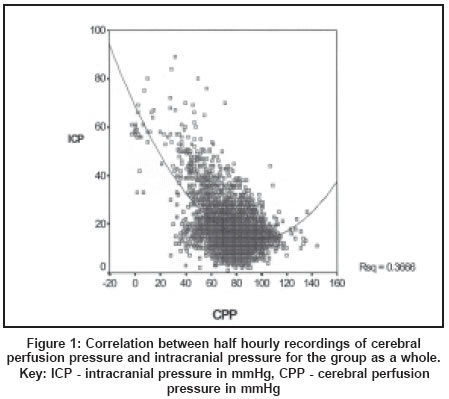
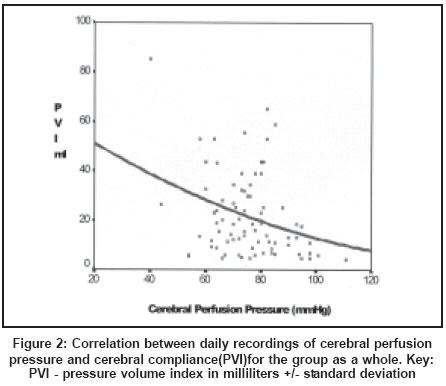
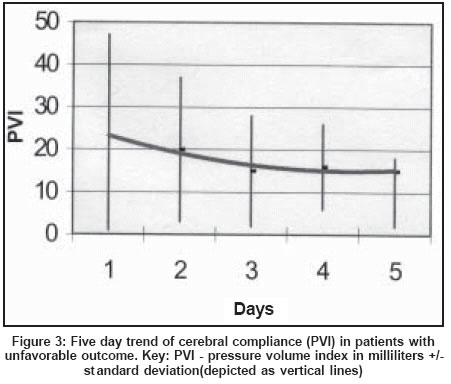
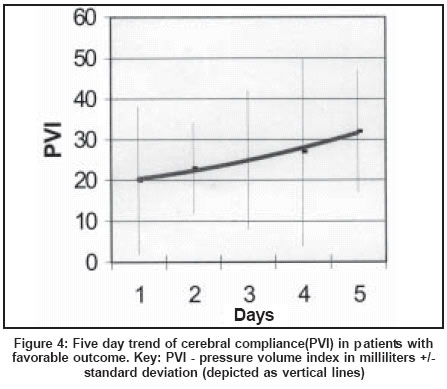
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 67-71 Original Article Cerebral perfusion pressure management of severe diffuse head injury: Effect on brain compliance and intracranial pressure Pillai S, Praharaj SS, Rao GSU, Kolluri VRS Departments of Neurosurgery, National Institute of Mental Health and Neurosciences, Bangalore Code Number: ni04016 Abstract Background: Cerebral perfusion pressure management (CPPM) is an accepted modality of treatment of severe diffuse head injury (SDHI). However, CPPM has the potential to cause transcapillary exudation in the presence of a disrupted blood brain barrier and can lead to further increase of intracranial pressure (ICP) and worsening of compliance. Aims: This study attempts to evaluate the effect of both transient and prolonged changes in cerebral perfusion pressure (CPP) on ICP and cerebral compliance as measured by the Pressure Volume Index (PVI), and to correlate changes in PVI with outcome at 12 months using the Glasgow Outcome Score. Settings and Design: Prospective study in a neurosurgical ICU. Material and Methods: Twenty-seven SDHI patients managed using standard protocol to maintain CPP above 70 mmHg. Mean arterial pressure (MAP), ICP and CPP were monitored every half-hour. Daily monitoring of the PVI and ICP was done before, and after the induced elevation of MAP using IV Dopamine infusion. The relationship between CPP, MAP, ICP, PVI and outcome was evaluated. Statistical analysis used: The paired and independent samples T-test, and the Pearson correlation coefficient. Results: CPPM rarely leads to progressive rise in ICP. Maintaining CPP above 70mmHg does not influence ICP or PVI. Transient elevations in CPP above 70mmHg may produce a small rise in ICP. Trend of change in PVI influenced outcome despite similar ICP and CPP. Conclusion: Elevating the CPP above 70mmHg does not either reduce the ICP or worsen the compliance. Monitoring changes in compliance should form an integral part of CPPM.Introduction Autopsy studies[1] have demonstrated ischemic brain damage in 88-92% of patients who died following head trauma. Maintenance of high cerebral perfusion pressure (CPP) in severely head-injured patients reduced the intracranial pressure (ICP) through the "autoregulatory vasoconstrictive cascade"[2] and improved outcome[3] when compared to the ICP-based techniques represented in the Traumatic Coma Data Bank (TCDB) data.[4] However, as the blood brain barrier is generally impaired in patients with severe head injury, a high CPP has the potential to increase transcapillary exudation and can lead to progressive vasogenic brain edema, decreased cerebral compliance and elevated ICP.[5] Several authors have reported that changes in CPP do not influence cerebral compliance as measured by the Pressure Volume Index (PVI) when autoregulation is intact.[6],[7],[8],[9] Gray and Rosner[10] found a positive correlation between CPP and PVI in experimental animals, and Rosner et al[3] found a similar correlation during CPP management of head injured patients. However, all these studies involved inhomogeneous groups of patients and they studied either the effect of transient changes in CPP or of sustained elevation in CPP. Our study attempts to evaluate the effect of both transient and sustained elevations of CPP on PVI and ICP in a homogenous group of patients with SDHI and to compare the changes in compliance in patients with favorable outcome to those who had unfavorable outcome. This study also attempts to see if the effect of elevating CPP depends on the initial level of CPP. Material and Methods Twenty-seven consecutive adults with SDHI, with a highest post-resuscitation Glasgow Coma Score (GCS)[11] of 8 or less, were included in this study. Patients with an operable mass lesion more than 1 cm in diameter on their initial cranial CT scan, associated systemic injuries, uncontrolled hypotension at the time of admission, and those with fixed dilated pupils and absent oculocephalic reflex were excluded. Informed consent for inclusion in the study was obtained from the relatives of the patients. Ethical clearance was obtained. Patients were constantly sedated and were mechanically ventilated to maintain a targeted PaCO2 of 30-35 mmHg and PaO2 of 100 mmHg. All patients were nursed in the supine position without elevation of the head end. Central venous pressure (CVP) was monitored and maintained at 10-12 cm H2O. One liter of colloids (hydroxy-ethyl starch, plasma, blood) and additional crystalloids (normal saline or dextrose saline) were transfused every day. Mean arterial blood pressure (MAP) and intracranial pressure (ICP) (using an external ventricular drainage catheter-EVD) were monitored continuously for 5-6 days. Monitoring was stopped prior to that if the patient improved to the extent of obeying requests and ICP had remained normal for 48 hours and was continued beyond that if thought essential for ICP management. The MAP, ICP and CPP (MAP-ICP) were recorded at half-hourly intervals. Therapy was adjusted every half hour to achieve a target CPP of 70 mmHg after ensuring the adequacy of sedation and euvolemia. The therapeutic ladder consisted of three sequential steps: 1] CSF drainage from the EVD, 2] 20 g bolus doses of mannitol up to a maximum dose of 200g /day, and 3] raising MAP using an intravenous infusion of Dopamine (5-15 µgm/kg/min). The intensity of therapy was increased every half hour to achieve the target CPP [1] / [1]+[2] / [1]+[2]+[3]. The cranial CT scan was repeated on Day 5 or earlier if ICP remained persistently high. The outcome was assessed at 12 months using the Glasgow Outcome Scale,[12] with Good Recovery and Moderate deficit classed as favorable and the rest as unfavorable. Pressure-volume studies, and the effect of transient induced hypertension Results The mean age of the 27 patients was 31+/-9 years (range 21-60 years). GCS was 3-5 in 9 and 6-8 in 18. The mean duration of ICP and CPP monitoring was 5 +/- 1 day. The patients were categorized into 4 groups based on Marshall′s classification of Diffuse Brain Injury (DBI)[15] and included those with Normal CT scan (DBI 1, n = 10), Diffuse Axonal Injury (DBI 2, n = 5), Diffuse Brain Swelling (DBI 3, n = 10), Brain swelling with shift (DBI 4, n = 2). All patients, except two with DBI 1 and 2, had recordings of ICP > 20mmHg, which required treatment with CSF drainage. Thirteen patients had a favorable outcome, and 14 patients had an unfavorable outcome. Five patients died, one due to sepsis (DBI 1) and the others due to uncontrolled raised ICP (DBI 3/4). The correlation between the half-hourly recordings of CPP and ICP for the group as a whole is shown in [Figure - 1]. The data was divided into three groups based on the level of CPP - Group A: 40-69 mmHg, Group B: 70-90 mmHg and Group C: > 90 mmHg. The data below CPP of 40 mmHg were excluded as they represent terminal events and therefore were of little importance in real treatment. The Pearson correlation coefficient was significant for Group A (-0.6), but was not significant for the other groups. The inverse correlation in Group A is a reflection of an uncontrolled rise in ICP leading to fall in CPP. In order to evaluate the effect of CPP management protocol on the ICP over the period monitored, the slope of the linear regression line of change in CPP and ICP was calculated for each of the patients. The mean slope of CPP (0.75 +/- 2.7, Standard error = 0.55) was not significantly different from the mean slope of ICP (0.41 +/- 1.65, Standard error = 0.33) (paired samples T-test). The daily recordings of PVI were correlated with the corresponding CPP values [Figure - 2]. The data was divided into three groups based on the level of CPP - Group A: 40-69 mmHg, Group B: 70-90 mmHg and Group C: >90 mmHg. The Pearson correlation coefficient was significant only for Group A (-0.5). In order to see if the effect of transient induced hypertension is dependent on the initial level of CPP, we divided the data into two groups based on initial CPP above 70 mmHg (n=50) or below 70 mmHg (n=24). When CPP was elevated from 80+/-9 to 97+/-11 mmHg, the ICP increased from 13+/-5 to 15+/-6 mmHg (P=0.001) but the PVI did not change significantly (21+/-16 to 22+/-18 ml) whereas when CPP was elevated from 61+/-7 to 77+/-15 mmHg, there was no significant change in either the ICP (17+/-6 to 18+/-6 mmHg) or the PVI (24+/-20 to 21+/-15ml) (paired samples T-test). The PVI of patients who improved was compared with that of patients who failed to improve. In patients who had an unfavorable outcome the mean PVI for the day fell from 23 +/- 22 ml on Day 1 to 15 +/- 13 ml on Day 5 [Figure - 3]. In contrast, the PVI of patients with a favorable outcome rose from 20 +/- 18 ml on Day 1 to 32 +/- 15 ml on Day 5 [Figure - 4]. There was no difference (Independent samples T-test) between the mean PVI for the two groups on Days 1 to 4 (P = 0.7). However, on Day 5 the patients who went on to have a good outcome were found to have a higher PVI (better compliance) compared to those who had an unfavorable outcome (P = 0.05). On Day 5, there was no significant difference in the CPP and ICP between the patients who improved and those who did not improve - mean CPP was 78 +/- 7 mmHg and 76 +/- 9 mmHg respectively, and mean ICP was 19 +/- 8 mmHg and 21 +/- 1 mmHg respectively. Moreover, the therapy intensity level of these patients was not significantly different. A linear regression line of the daily changes in the PVI of each of the patients was drawn and the slope of this line was calculated. The Pearson correlation coefficient of this slope and the GOS was 0.513. The mean slope for patients with unfavorable outcome (-11.4 +/- 19) was significantly different from that for patients with favorable outcome (1.3 +/- 5.6) (independent samples t-test for equality of means, P = 0.05). Discussion All patients had severe diffuse brain injury, hence the confounding effect of focal areas of abnormal autoregulation and mass-effect was avoided. Patients with DBI 1 and DBI 2, based on the initial CT scan, were included because even they can develop episodes of raised ICP (13/15 in the present study) and according to the "complex vasodilatory/ vasoconstrictive cascade" theory[2] such transient episodes of raised ICP can precipitate plateau waves. The study did not incorporate a control arm of patients in whom compliance could be measured without manipulating the CPP and hence, cannot demonstrate a direct cause-effect relationship between CPPM and cerebral compliance. Studies[2],[3],[7],[16] have demonstrated that elevation of CPP by inducing systemic hypertension can lead to progressive reduction in the ICP. The opposite viewpoint is that CPPM is dangerous because of the potential to induce vasogenic edema and raise the ICP.[5],[17],[18],[19],[20] Our study, on the contrary, shows that elevating CPP above 70 mmHg does not either enhance ICP control or raise the ICP. This is probably because we did not attempt to elevate the CPP beyond our moderate target level even when a fall in ICP was not achieved (unlike the CPP of even 110-130 mmHg that was reported in the studies quoted above). Thus, CPPM with a moderate CPP target is safe. Portella et al[21] using the Spiegelberg catheter to evaluate the correlation between CPP and compliance found that there was no relation between them when the ICP < 20 mmHg and that they varied directly when the ICP > 20 mmHg, irrespective of CPP being above or below 60 mmHg. Our study, on the contrary, demonstrates that CPPM causes a fall in PVI only when the CPP remains below 70 mmHg. This is probably the result of passive vasodilatation due to impaired autoregulation leading to increase in cerebrovascular volume and worsening cerebral compliance when CPP remains in the 40-69 mmHg range. CPPM does not influence the cerebral compliance once the CPP is elevated above 70 mmHg. This is probably because above a CPP of 70 mmHg, pressure autoregulation is more effective and causes reduction in cerebrovascular volume which balances any increase in the transmural transmission of pressure in the cerebral vasculature which is responsible for the change in compliance.[22] Thus, CPPM with a target of 70 mmHg helps prevent a deterioration of cerebral compliance. Bouma et al[7] demonstrated that when autoregulation is intact transient elevation of MAP by about 30% does not change ICP, but in the absence of autoregulation, ICP varies directly with MAP. In our study, transiently elevating the CPP from a level above 70 mmHg resulted in a rise in ICP which in spite of being statistically significant is not very large in the clinical context, whereas elevation in CPP from a level below 70 mmHg did not lead to a significant change in the ICP. Lang et al[23] studied the relationship between MAP, CPP, ICP, transcranial Doppler peak flow velocity (TAP) and brain tissue oxygen reactivity (Ptio2) during stepwise increase in CPP using noradrenaline infusions in patients with head injury. They demonstrated a TAP and Ptio2 plateau between CPP of 70-90 mmHg, suggestive of intact autoregulation in this range of CPP. They reported a significant rise in ICP when CPP was elevated above 90 mmHg (P=0.05). However, these changes in ICP are of the order of 1-2mmHg when the CPP was 50-110mmHg and only beyond CPP of 110 mmHg is there a really steep rise in ICP. These findings are very similar to those in the present report. Minassian et al[24] confirm that a hypertensive challenge during CPPM will not cause significant rise in ICP, irrespective of the autoregulatory status, in most patients; though rarely, in patients with ICP > 20 mmHg, there may be a rise in ICP by > 5 mmHg. We, therefore, suggest that elevations of CPP above 70 mmHg are not beneficial or prudent. Several studies involving pentobarbital-anesthetized animal models[8],[25],[9] have demonstrated that when autoregulation is intact, changes in CPP did not lead to changes in PVI. Outside the autoregulatory range, changes in PVI became inversely related to CPP. Contrary to these reports, Gray and Rosner[10] found a significant positive correlation between PVI and CPP within the autoregulatory range in methohexital-anesthetized cats. Below the autoregulatory range PVI was again found to increase as CPP fell because of vaso-collapse. Bouma et al,[7] demonstrated in 47 severely head injured patients that when autoregulation was intact a rise in CPP of about 30% resulted in only small and statistically insignificant increases in PVI. In the absence of autoregulation PVI became inversely related to the CPP. Contrary to the above reports, transient elevations in CPP did not cause a change in the compliance in any of our patients. Kosteljanetz[26] has suggested that changes in PVI reflect protracted changes in CSF absorption and storage rather than transient vascular changes. This theory can explain why moderate changes in MAP in our study did not induce changes in the compliance. Studies[13],[27],[28],[29],[30] show that a low compliance is associated with higher risk of raised ICP and poor outcome. In the present study there was a decrease in cerebral compliance of patients who had an unfavorable outcome, whereas patients who improved had an increase in compliance. This difference in outcome did not depend on the initial PVI, which varied considerably, but on the trend of change in compliance. This finding contradicts the report by Maset et al[13] who said that patients with a low initial PVI had an unfavorable outcome and vice versa. Simulation studies[16] provide evidence that PVI is not a static physical property of the craniospinal space but a complex interaction of the CPP and autoregulatory status. Therefore if CSF "absorption" is maintained by ventricular drainage and if CPP is maintained at a high level then a low PVI may not lead to progressive intracranial hypertension. Therapy in patients with diffuse head injury should be directed at increasing the PVI in addition to maintaining a CPP consistently around 70 mmHg and a normal ICP. Probably, patients with decreasing PVI in spite of a normal ICP and CPP will benefit from more frequent and a longer period of ventricular CSF drainage to counter the high CSF outflow resistance seen in them and to encourage bulk-flow clearance of cerebral edema fluid by the ventricular route.[13],[26] Individual values of PVI can vary widely, hence, we suggest that only the trend of changing PVI rather than a particular "cut-off" value should be used to adjust therapy. Steiner et al[31] continuously recorded the cerebrovascular pressure reactivity index in order to identify the optimum CPP in patients with head injury. They found that this can vary from 60-85 mmHg in individual patients and the outcome at 6 months was poor if the actual CPP varied more than 5 mmHg above or below the optimum CPP. Their findings illustrate the difficulty in recommending the ideal target for CPPM. Our study suggests that CPPM targeted at 70 mmHg is safe with respect to ICP and cerebral compliance, but its effectiveness in reducing ICP is debatable. Further studies are required to evaluate the benefit of increased frequency and duration of CSF drainage in patients showing a trend of worsening compliance despite normal ICP and CPP during CPPM. Conclusion CPP management is a relatively safe modality of treatment of severe diffuse head injury. Cerebral compliance worsens only when the CPP remains persistently below 70 mmHg. Elevating the CPP significantly above 70 mmHg does not provide any additional benefits with regard to ICP control. One must be vigilant about the status of cerebral compliance during CPP management because in some patients a progressive decrease in the compliance of the brain occurs even when the CPP and ICP are relatively normal and this is associated with an unfavorable outcome. Hence, monitoring of the trend of change in compliance (PVI) should form an integral part of CPP management. CSF drainage should probably continue till compliance improves. Acknowledgements The efficient work of the neurosurgical ICU nurses is deeply appreciated. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04016f3.jpg] [ni04016f4.jpg] [ni04016f2.jpg] [ni04016f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}