 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
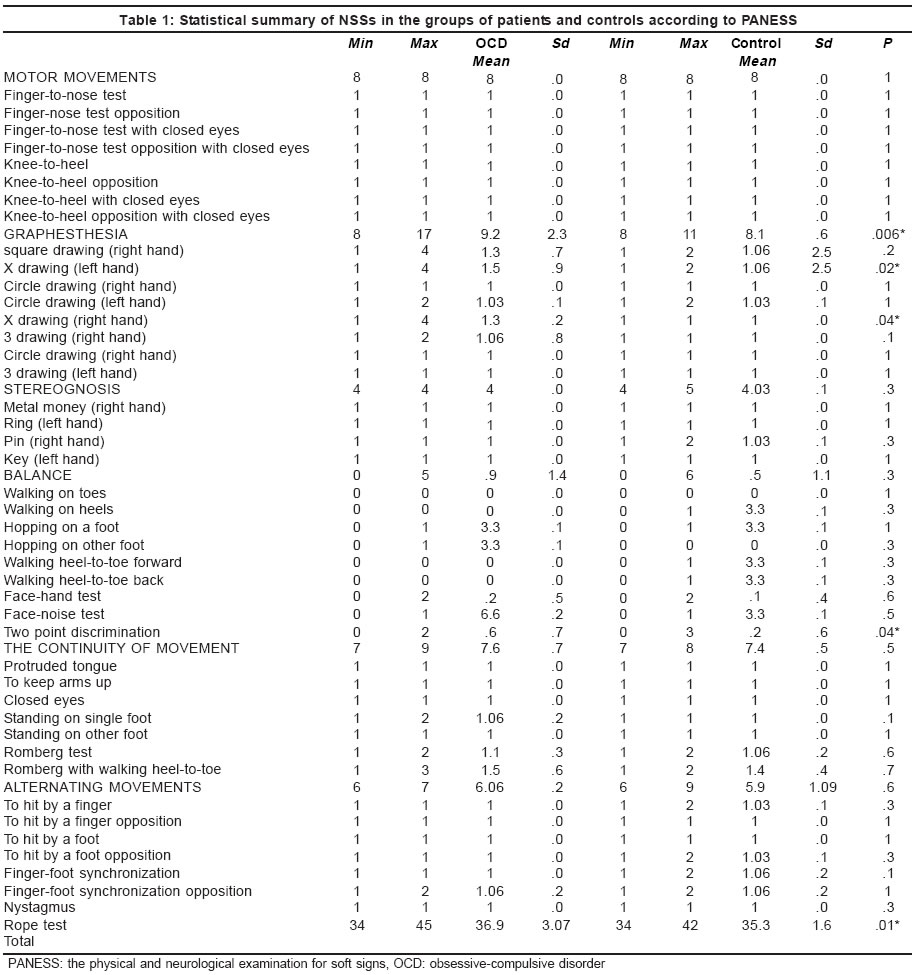
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 72-75 Original Article Neurological soft signs in obsessive-compulsive disorder Guz H, Aygun D Ondokuz Mayis University, Medical School, Departments of Psychiatry, Samsun Code Number: ni04017 Abstract Background: Neurological soft signs (NSSs) are defined as abnormal motor or sensory findings, including involuntary movements, a variety of dispraxia, difficulties in performing rapid alternating movements, difficulties in two-point discrimination, and graphesthesia in a person without a neurological disorder which can be determined as its focus. Aims: to investigate the relationship of NSSs with obsessive-compulsive disorder (OCD). Settings and Design: This study was designed in the Psychiatry Polyclinic of Ondokuz Mayis University Hospital. After signing an informed consent form, all the subjects were divided into 2 groups: (1) the patient group and (2) the control group. Material and Methods: Thirty consecutive patients presenting with DSM-IV OCD were included in this study. The control group consisted of 30 healthy subjects without a psychiatric/neurological disorder. All subjects underwent a physical and neurological examination for soft signs (PANESS). Statistical analysis used: The Mann-Whitney U test was used for statistical analysis of data. Results: It was seen that graphesthesia, two-point discrimination, and total PANESS scores were significantly higher in the group with OCD than the control group. In other NSSs, there was no significant difference between the patient and control groups. Conclusions: Unlike some studies, in the present study, the difference between the groups in graphesthesia compared to other NSSs was significant. The results of this preliminary study suggest that there is a relationship between NSSs and OCD. We think that NSSs may point to a structural brain abnormality in patients with OCD.Introduction Neurological soft signs (NSSs) are defined as motor or sensory disorders (e.g. difficulties in two-point discrimination and graphesthesia), without a structural lesion in the central nervous system (CNS).[1],[2],[3],[4],[5] There are many controversial reports in the literature about the relationship of obsessive-compulsive disorder (OCD) to NSSs.[1],[2],[3],[4] Stein et al[1] found no significant differences between the patients with OCD and normal controls for both total NSS scores and sensation. Hollander et al[3] reported that there is a significant difference between patients with OCD and normal controls in total NSS scores, but not in sensory abnormalities. However, they reported that compared with other psychiatric groups, the OCD patients had more graphesthesia and involuntary movements. On the other hand, Bolton et al[2] found that sensory integration did not differ significantly in the OCD group from those in the schizophrenia group. Thus, it is also controversial whether there is a specificity of NSSs for OCD.[2],[3] Additionally, their neurological basis and etiology is still uncertain.[3] This study aimed to investigate whether there is a significant difference between patients with OCD and healthy persons in the frequency of NSSs, especially sensorial impairment, and a role of NSSs in the pathophysiology of OCD, for example, their association with subsequent neuropsychiatric symptoms (i.e. a neuropsychiatric impairment) as to be in OCD; therefore, whether NSSs point to a structural lesion in addition to non-structural damage of the brain. We hypothesized that NSSs may point to not only a functional involvement of the brain but also to a structural lesion which cannot be showed by classical neuroimaging studies, that the affected regions of the brain for NSSs may resemble those in OCD, and that NSSs may be followed by the symptoms of OCD. Material and Methods Thirty consecutive patients presenting with DSM-IV OCD were included in this study. After signing an informed consent form, the subjects were divided into 2 groups: (1) the patient group, and (2) the control group. The control group consisted of 30 healthy subjects working in the hospital without a psychiatric/neurological disorder. They were paired with those in Group 1 according to age, sex, and hand dominance. Nneurological and physical examination, and laboratory studies [i.e. routine blood examinations and cranial computed tomography (CT-scan)] of the subjects were performed. The exclusion criteria included anoxia or hypoxia during birth; the presence of a major medical disorder or neuropsychiatric symptoms secondary to a metabolic disorder or structural lesion; consuming alcohol or other substances for the last 2 months; a history of receiving any drug including antidepressant and anxiolitic in the control group; a family history of any psychiatric disorder in the control group; any comorbid psychiatric disorders in the subject population (because comorbid psychiatric disorders are likely to influence the NSSs); and the presence of abnormal findings in routine blood examinations and on CT scan studies. During the study period, all patients were taking a selective serotonin re-uptake inhibitor; however, no patient had any behavioral therapy. The patients and controls underwent a physical and neurological examination for soft signs (PANESS) by a psychiatrist (HG).[5] The PANESS scores were not evaluated blind to diagnosis. However, all the subjects were examined again by a neurologist for the NSSs but he did not know the subjects′groups. This scale, which consisted of 43 components was used for the assessment of main motor movements, graphesthesia, stereognosis, balance, the continuity of movement, alternating movements, and nystagmus. In both, the patients and the controls, total scores were calculated according to this scale. The Mann-Whitney U test was used for statistical analysis of data. A P >0.05 was considered statistically insignificant. Results The patient and the control groups consisted of 11 females and 19 males each. The mean age of the patients was 36.3 ± 8.8 years. The mean age of the control subjects was also 36.3 ± 8.8 years. In both the patients and the control subjects, the number of persons with left-hand dominance was only one (total 2 persons). The mean duration of illness was 8.2 months (range, 6 to 14). When the groups were compared for PANESS scores, it was seen that graphesthesia, two-point discrimination, and total PANESS score were significantly higher in the group with OCD than the control group (P = 0.006, 0.04, and 0.01, respectively). For other characteristics, there was no significant difference between the patient and control groups (P > 0.05; [Table - 1]. There was no difference between females and males in the number of NSSs in both the groups (P > 0.05). All patients had normal CT scan findings. Discussion In the present study, we found significant differences in total soft sign scores, graphesthesia, and two-point discrimination between the OCD patients and the control subjects. The graphesthesia, two-point discrimination, and total PANESS scores were significantly higher in the OCD group than the control group. For other characteristics, there was no significant difference between the patient and control groups. Hollander et al[3] reported that there were significant abnormalities in total NSSs, fine motor co-ordination including finger-to-finger, tongue twister, and mirror movement abnormalities, abnormal involuntary movements, and visiospatial function (e.g. cube-drawing) in adult patients with OCD when compared with normal controls. They found at least one abnormal soft sign in 39 out of 41 patients. Unlike the present study, they did not find a difference between the patient and control groups in sensory abnormalities (e.g. graphesthesia). However, total NSSs resembled our result. Stein and co-workers[1] found no significant differences between the patients with OCD and normal controls in both total NSS scores and sensation. On the other hand, Hollander et al[3] reported that compared with other psychiatric groups, the OCD patients had graphesthesia and involuntary movements more than other NSSs. However, Bolton et al[2] found that the levels of NSSs in the OCD group did not significantly differ from those in the schizophrenia group in sensory integration. Finally, we think that the relationship of graphesthesia to OCD was stronger than that of other NSSs. The neurological basis and etiology of NSSs is obscure.[3] However, it has been pointed to the presence of a genetic component to NSSs.[6],[7] On the other hand, in some studies, authors have suggested that that NSSs may reflect a genetic predisposition underlying the development of OCD and schizophrenia.[8],[9] Thus, it has been understood that subjects with NSSs are likely to develop subsequently a psychiatric disorder such as OCD or schizophrenia. Whereas Hollander et al[3] have reported that NSSs appear as the indicators of non-structural damage of the brain, which may cause neuropsychiatric symptoms (i.e. neuropsychiatric impairment). Some studies have shown that abnormalities in some regions of the brain including the basal ganglia, the frontal lobe, and the right-hemisphere are related to OCD.[10],[11] Additionally, surgical interruption of frontal, cingulum, or related fibers has been found effective in OCD treatment.[12] Graphesthesia and difficulties in discerning two-point discrimination are sensorial disorders considering a hemispheric cortical involvement.[13] We think that NSSs may point to not only a functional involvement of the brain but also to a structural lesion, and that the affected regions of the CNS in NSSs will probably resemble those in OCD. The presence of an association between gender and the number of NSSs in patients with OCD is a controversial topic in the literature.[14],[15],[16],[17] In our study, there was no difference between males and females for NSSs in patients with OCD. Conclusion Unlike some studies, in the present study, the difference between the groups in graphesthesia compared with other NSSs was significant. There is already much information on the structural and functional brain abnormalities in OCD. We think that NSSs are also likely to related to both structural and functional brain abnormalities that the affected regions of the brain for NSSs probably resemble those in OCD, and that NSSs may be followed by the symptoms of OCD. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04017t1.jpg] |
| |||||||||

{kind=link}