 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
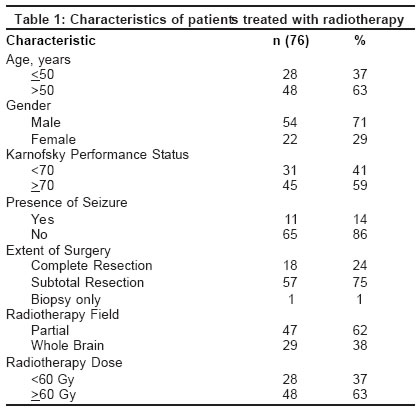
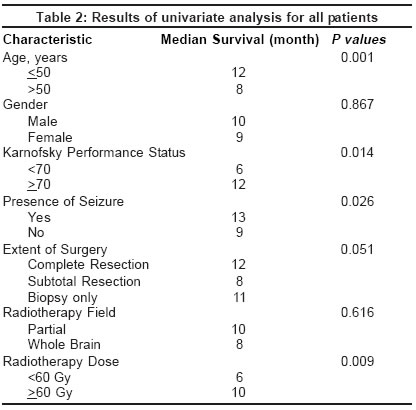
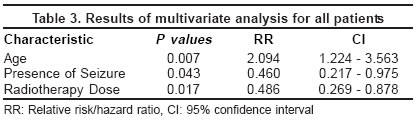
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 76-78 Original Article Prognostic significance of seizure in patients with glioblastoma multiforme Ozbek N, Cakir S, Gursel B, Meydan D Ondokuz Mayis University, School of Medicine, Department of Radiation Oncology, Samsun Code Number: ni04018 Abstract Background: Several prognostic factors have been described but there are few studies evaluating the prognostic importance of seizure in patients with glioblastoma multiforme (GBM). Aims: To evaluate the prognostic importance of seizure at the time of the diagnosis of glioblastoma multiforme (GBM) and compare it with other known prognostic factors. Settings and Design: Between January 1994 and December 2000, 81 patients underwent irradiation for intracranial GBM at our institution. The criteria for inclusion in this study were biopsy-proven GBM, being treated for primary disease. Seventy-six patients were retrospectively evaluated and the remaining five patients could not be enrolled due to lack of details. Material and Methods: The prognostic importance of age, sex, performance status, a history of seizure at diagnosis, extent of surgery, radiotherapy field and dose were studied. Statistical analysis: The Kaplan-Meier method, the Log rank test, the Cox proportional hazard model and the Mann-Whitney U test were used for statistical analysis. Results: Survival at first and second years was 19.74% and 4.81%, respectively. Univariate analysis revealed age, performance status, history of seizure, and radiotherapy dose as significant prognostic factors and with multivariate analysis age, history of seizure and radiotherapy dose were positive prognostic factors. Conclusion: This study concluded that in GBM, history of seizure prior to diagnosis of GBM was a positive prognostic factor.Introduction The patients with glioblastoma multiforme (GBM) have a median survival between 9-12 months.[1],[2],[3],[4] Despite its uniformly lethal course, the survival of patients with GBM varies considerably. The identification of prognostic factors could potentially increase prognostic accuracy and might also be helpful for designing clinical trials of novel therapies. A majority of studies have proven the presence of neurological symptoms to be poor prognostic factors for survival. The only exception to this was the presence of seizure, which appeared to be a favorable prognostic factor.[5] However, there were a few studies evaluating the prognostic importance of seizure in the survival of patients with GBM. In the present study, we retrospectively analyzed the prognostic importance of seizure at initial presentation of patients with GBM. Material and Methods Between January 1994 and December 2000, 81 patients underwent irradiation for intracranial GBM at our institution. The criteria for inclusion in this study were biopsy-proven GBM, being treated for primary disease. Seventy-six patients were evaluated and the remaining five patients could not be enrolled due to lack of records. The performance statuses of the patients were scored via the Karnofsky Performance Status (KPS) scale. KPS was <70 for 31 patients and > 70 for 45 patients. There were 11 patients with a history of seizure prior to diagnosis and 65 patients with no such history. The interval between the onset of symptoms of GBM and tissue diagnosis was considered as the duration of symptoms. The mean duration of symptoms in patients with history of seizure was 78.9 days (8-240 days), in patients without seizure was 57.5 days (7-365 days). Biopsy alone was performed in one, subtotal resection in 57, and complete resection in 18 patients. Radiotherapy was delivered by Cobalt 60. Portals and techniques of radiation varied with the tumor location and size. The target volume was based on the preoperative brain computed tomography or magnetic resonance imaging. If edema was more than 2/3 of a hemisphere, whole brain was irradiated. The field size was referred to as "partial" when the initial target volume included the contrast-enhancing lesion and surrounding edema plus a two-cm margin. The reduced volume was used after 46 Gy in whole brain irradiated patients (n= 29) and 50 Gy in partially irradiated patients (n=47). Reduced volume included the contrast-enhancing lesion plus a two-cm margin. Radiotherapy was given with 2 Gy/day, five days a week and total median dose of 60 Gy (24-66 Gy). Radiotherapy dose was < 60 Gy for 28 patients and > 60 Gy for 48 patients. The lower total doses were seen in patients who experienced disease progression early in therapy. The patients′tumor, and treatment-related variables are shown in [Table - 1]. All patients were controlled weekly during treatment and at two-months′intervals thereafter. Imaging was obtained periodically and/or as indicated by changes in the neurological or performance status. Statistical Analysis: Survival was calculated from the time of the initial operation until the patient died or until the final analysis. Survival rates were determined by the Kaplan-Meier method and differences were analyzed by the Log rank test. Uni-and multi-factor analysis was carried out using the Cox proportional hazard model. The duration of symptoms between the groups was analyzed with the Mann-Whitney U test.[6] Results The median age of the patients was 55 years (19-86 years); 28 patients were < 50 years and 48 patients were > 50 years old. There were 54 males and 22 females. Median actuarial survival for the entire population studied was 10.3 months. Survival at first and second years was 19.74% and 4.81%, respectively. Four patients were alive at the time of final analysis. Age <50 years (P=0.001), KPS score > 70 (P=0.014), presence of a history of seizure prior to diagnosis (P=0.026) and radiation dose (P=0.009) were associated with increased median survival time in univariate analysis [Table - 2]. Multivariate analysis displayed that age<50 years (P=0.007), presence of seizure history prior to diagnosis (P=0.043) and radiotherapy dose (P=0.017) were favorable independent risk factors for median survival time [Table - 3]. The mean duration of symptoms in the groups with and without history of seizure was 57.52 ± 63.78 days and 78.91 ± 76.14 days, respectively (z=-1.097, P=0.272). Discussion In recent years several prognostic variables have consistently been shown to be important in patients with GBM. There was a general consensus about the prognostic value of age, performance status, and extent of surgical resection in GBM, with every published report confirming the strong impact of these variables on patient survival.[4],[7],[8],[9] In our study, the age of the patient, in agreement with many other studies,[2],[10] was the most significant factor in GBM. Salminen et al[11] like our results, demonstrated that gender did not predict outcome. KPS emerged as a significant prognostic factor.[7],[9] The present analysis also showed that KPS was a significant prognostic factor. There was no clear consensus about the status of the extent of surgical resection in the current literature. Miller et al[8] suggested that the extent of surgery did not predict outcome. Vecht et al[12] and Shibamoto et al[3] showed that extensive surgery was correlated with a longer survival time compared to limited surgery. The findings of our study showed that extent of surgery did not prove to be a statistically significant prognostic factor. This conclusion might be affected by the groups′ sample sizes. Shibamoto et al,[3] Kleinberg et al[13] and our study demonstrated that GBM patients with whole brain irradiation had a survival rate similar to that of those treated with partial field treatment. The preference of whole brain irradiation was not a treatment policy but result of diffuse edema. Some authors reported that higher doses could have an independent role in prolonging survival time.[1],[14] The others[15],[16],[17] reported no difference in outcome between patients receiving 60 Gy and higher doses. The results of our study suggested that higher doses achieved better results than lower doses. Headache was found to be the most frequent symptom and seizure was the second most common complaint at the time of diagnosis in patients with GBM. It has been reported that more than one-third of all patients suffered from seizures,[18] however, seizure had not been evaluated in most of the studies. When evaluating the presence of seizure, some studies reported a favorable effect; whereas some others found it had no effect on prognosis. McKeran and Thomas[19] reported prolonged history of seizure being associated with a better prognosis. Curran et al[20] showed that seizure did not play a significant role. Winger et al[4] found that seizure as the initial symptom was statistically significant in the univariate analysis but they were unable to demonstrate that seizure was a significant independent prognostic factor for patients with anaplastic glioma. Miller et al[8] reported that the patients with seizure had a better survival time both with univariate and multivariate statistical analysis. They suggested that seizure might lead to an earlier diagnosis in the course of the disease and thereby better prognosis In another study, The Brain Tumor Study Group (69-01)[21] screened patients with brain tumors for prognostic factors and found that seizure was a favorable prognostic factor. In our study, the median survival time of 11 patients with a history of seizure was 13 months, whereas it was nine months in 65 patients with no such history. Our results showed that in GBM, a history of seizure prior to diagnosis has positive prognostic significance. The duration of symptoms didn′t show a statistically significant difference between the two groups. According to our results it′s hard to say that longer survival in the patients with seizure was the effect of early diagnosis. This prolonged survival in the seizure group might be associated with factors such as tumor localization and size, but our study group was very small to identify these. In conclusion, this study suggested that history of seizure prior to diagnosis was significantly associated with prolonged survival in patients with GBM. Estimating the prognostic factors correctly would help us to make a better choice of subgroups of patients which were to be included in subsequent studies and to ensure the effectiveness of new treatment modalities. This was a retrospective analysis with a small number of patients so this subject has to be further investigated with large study groups. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04018t2.jpg] [ni04018t3.jpg] [ni04018t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}