 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
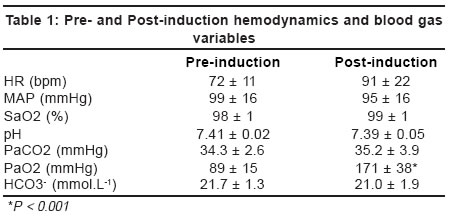
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 79-81 Original Article Cerebral blood flow velocity changes under nitrous oxide halothane anesthesia in patients with frontotemporal gliomas: A comparison of the normal and abnormal cerebral hemispheres Vajramuni GV, Umamaheswara Rao GS, Pillai SV National Institute of Mental Health and Neurosciences, Bangalore - 560029 Code Number: ni04019 Abstract Background: Regional differences in vascular response to anesthetic agents in brain areas with and without tumors have not been investigated till now. The existence of such differences may influence the regional distribution of cerebral blood flow under anesthesia. Material and Methods: In 8 patients with frontotemporal gliomas, middle cerebral artery blood flow velocity (Vmca), pulsatality index (PI) and resistance index (RI) were determined in the normal and pathological cerebral hemispheres before and after stable nitrous oxide-halothane anesthesia. Results: During halothane anesthesia, there was an increase in Vmca both in the normal cerebral hemisphere (69 ± 11 to 100 ± 38 cm/s; P = 0.05) and the hemisphere with tumor (65 ± 17 to 83 ± 28 cm/s; P = 0.04). A significant decrease in the pulsatality index and the resistance index was also observed in both the hemispheres (P < 0.05). The percentage changes of Vmca,, PI and RI in both the hemispheres after anesthesia were not significantly different. Conclusions: In patients with cerebral tumors, nitrous oxide-halothane anesthesia causes comparable changes of cerebral blood flow velocities in the hemisphere with tumor and the normal hemisphere.Introduction Inhalational anesthetics in current usage have varying levels of cerebral vasodilatory effect. Current literature does not clarify if there are any regional differences in the cerebral blood flow effects of inhalational anesthetics between normal areas and brain areas with tumor. If such differences exist, they may have major clinical implications similar to the steal and inverse steal phenomena caused by changes in arterial carbon dioxide pressure.[1] If the cerebral vasodilatory response to inhalational anesthetics is totally or partially impaired in brain areas with tumor, administration of inhalational agents could induce a steal phenomenon. The current study addresses this issue by comparing the cerebral blood flow velocity changes under halothane anesthesia in the normal cerebral hemisphere and the cerebral hemisphere with tumor in neurosurgical patients undergoing supratentorial craniotomy. Material and Methods In 8 patients with frontotemporal gliomas undergoing supratentorial craniotomy, baseline Transcranial Doppler (TCD) examination of the middle cerebral artery (MCA) on both the sides was carried out before the induction of anesthesia using an Ultramark 9 ultrasound system (Advanced Technology Laboratories Inc. USA). MCA was insonated through the transtemporal window according to the technique described by Aaslid et al[2] and the time averaged peak velocity (Vmca), Pulsatality Index (PI) and Resistance Index (RI) were recorded. Anesthesia was induced in all patients with morphine 0.2 mg.kg-1 followed by thiopentone 7 mg. Kg.-1 Endotracheal intubation was carried out after administering 0.15 mg.kg-1 of pancuronium bromide followed by intravenous lignocaine 1 mg.kg-1. Anesthesia was maintained by intermittent positive pressure ventilation with nitrous oxide in oxygen (60:40) and halothane 0.5% inspired concentration. Ventilation was adjusted to achieve normocapnia using Seimen′s Servo 900 D anesthesia ventilator. TCD examination was repeated after 15 min of stable anesthesia. Heart rate (HR), mean arterial blood pressure (MAP), end tidal carbon dioxide tension (PetCO2), oxygen saturation (SpO2) and arterial pH, PaO2, PaCO2 and bicarbonate were recorded both before induction of anesthesia and after stabilization of anesthesia. The hemodynamic parameters were monitored using a Datex Cardiocap II ® (Datex Instrumentarium, Finland) multichannel monitor and the blood gas analysis was carried out using a Radiometer ABL 330 blood gas analyzer (Radiometer, Copenhagen, Denmark).Statistics Results There were 7 male and 1 female patients in the study. Their mean age was 42 ± 19 years. Their pre- and post-induction hemodynamic and blood gas variables were comparable but for PaO2, which was higher after anesthesia because of the usage of higher inspired oxygen concentration under anesthesia [Table - 1]. Changes in TCD Parameters Discussion In this study in patients with frontotemporal gliomas, we showed that nitrous oxide - halothane anesthesia produced changes in MCA blood flow velocities and TCD indices of vascular resistance, which were similar between the normal cerebral hemisphere and the hemisphere with tumor. Vmca increased significantly and PI and RI decreased significantly in both the hemispheres. However, the percentage changes in Vmca, PI and RI were not different between the hemispheres. Differences in regional cerebral blood flow between normal brain and brain areas with tumor have been documented.[3],[4] Abnormal pressure autoregulation[5] and vascular response to carbon dioxide[1] have also been documented in brain regions with tumor. However, there are no studies documenting whether similar differences exist with regard to cerebrovascular response to inhalational anesthetics. If such differences in vascular reactivity exist, they may lead to major changes in the distribution of cerebral blood flow following administration of these anesthetics. Such redistribution of cerebral blood flow could have either a cerebral protective or ischemic effect depending on the relative effects of the anesthetic in the normal brain areas and the brain areas with tumor. TCD sonographic changes caused by inhalational anesthetics have been reported earlier.[6],[7],[8] However, in these studies, no specific attempt has been made to examine if there are any differences in the cerebral blood flow velocities between the cerebral hemispheres with and without pathology. Dong et al[9] observed a uniform 20% decrease in MCA blood flow velocity upon induction with thiopentone in patients undergoing microvascular decompression (non-tumor group) as well as in patients undergoing craniotomy for tumor removal (tumor group). In a subsequent study, the same group performed Doppler ultrasonographic examination of the right MCA during induction of anesthesia with thiopentone in 20 non-tumor and 85 tumor-bearing patients. MCA flow velocity decreased significantly with induction of anesthesia. The right MCA flow velocity was significantly higher in bilateral and right-sided tumor patients as compared to non-tumor patients. It was not significantly different between patients with left-sided tumors and no tumors. The limitation of this study is that the TCD examination was performed only on the right side, irrespective of the side on which the tumor was located. Secondly, the effect of the tumor on MCA blood flow velocity changes under anesthesia was evaluated by studying two different groups of patients (one group with tumors and another without tumors) and not by studying the normal and abnormal hemispheres of the same patient.[10] In addition, the above studies evaluated only the transient changes that took place during the induction of anesthesia. Changes that occur during the maintenance phase of anesthesia are more relevant from a practical standpoint as prolonged changes in the distribution of cerebral blood flow in this phase may have consequences leading to either cerebral protection or cerebral steal. In the current study, MCA blood flow velocities and TCD indices of cerebrovascular resistance (PI and RI) were measured in both cerebral hemispheres of the same group of patients. All patients in the study had a histologically similar parenchymal brain tumor (astrocytoma Grade II and III). The location of the tumor was also similar in all cases. Tumors with different histology may have differences in regional cerebral blood flow. The majority of intracranial tumors are relatively avascular and have correspondingly low cerebral blood flow values. Studies using Xe-133 and SPECT techniques have documented lower cerebral blood flow in the brain regions with parenchymal tumors when compared to normal brain.[1] Measurements performed in tumors such as meningiomas and metastases with prominent vascular features show evidence of increased blood flow.[1] By restricting the study to a single class of tumors with a similar location, we avoided discrepancies that could have arisen as result of the histological types and location of the tumors. In a recent study examining the effects of hyperventilation on nitrous oxide-induced increase in Vmca in cerebral hemispheres with and without tumors, nitrous oxide produced comparable changes in both the hemispheres (62 ± 14 to 74 ± 17 cm.s-1 on the healthy side and 72 ± 18 to 86 ± 16 cm.s-1 on the tumor side).[11] To our knowledge, the current study is the first to examine the relative changes in cerebral blood flow velocities between the healthy and tumor sides under inhalational anesthesia. The results suggest that the cerebral blood vessels react by vasodilation on both sides and there is no significant difference in the reactivity of the cerebral blood vessels between the two hemispheres as indicated by comparable changes in Vmca, PI and RI on both sides. In conclusion, in patients with frontotemporal gliomas, halothane anesthesia produced a similar increase in MCA cerebral blood flow velocity in the normal cerebral hemisphere and the hemisphere with tumor. Future studies with varying concentrations of inhalational agents and more direct techniques of measurement of cerebral blood flow are required to examine the regional differences in vascular reactivity to inhalational anesthetics and their implications in the management of patients undergoing surgery for intracranial tumors. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04019t2.jpg] [ni04019t1.jpg] |
| |||||||||

{kind=link}
{kind=link}