
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 1, 2004, pp. 82-86
|
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 82-86
Original Article
Clinico-pathological study of cerebral aneurysms
Rajesh BJ, Sandhyamani S, Bhattacharya RN
Departments of Neurosurgery, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum
Correspondence Address:Departments of Neurosurgery, Sree Chitra
Tirunal Institute for Medical Sciences and Technology, Trivandrum bjraj1@sctimst.ker.nic.in
Code Number: ni04020
Abstract
Aims and Objectives: A clinico-pathological study of cerebral aneurysms
was undertaken to understand the histopathogical nature of the lesions
and to ascertain possible etiological risk factors. Material and Methods:
Of the 255 cases of cerebral aneurysms operated upon at our Institute during
the two-year period between Jan 1999 to Dec 2000, a detailed study was
conducted on 57 cases where the aneurysm sac could be excised and subjected
to histopathological examination. Aneurysm sacs were fixed in 10% buffered
formaldehyde and processed through graded alcohol. Paraffin-embedded sections
were examined, using hematoxylin and eosin, Verhoeff van Gieson’s and toluidine
blue staining techniques. Histopathological observations were analyzed
and correlated with clinical features. Results: The ages of the patients
ranged from 17-65 years and there were 33 males and 24 females. Twenty-six
patients were chronic smokers and 19 patients had hypertension. There were
54 saccular and 3 fusiform aneurysms, predominantly involving the anterior
circulation (52 cases) than posterior circulation (5 cases). In 35 cases,
histopathological studies demonstrated mucoid deposits between hyperplastic
cellular elements in the true and false aneurysm wall and/or parent artery
or vasavasora. The changes were associated with dystrophic changes in the
internal elastic lamina. Conclusion: Besides significant risk factors like
smoking and hypertension, such mucoid vasculopathic changes may have predisposed
vessels to structural weakness and aneurysm formation in our patients.
Introduction During the last 25 years, besides mycotic aneurysms,[1],[2],[3] a large number of cerebral aneurysm cases with no definite cause, were encountered at Sree Chitra Tirunal Institute for Medical Sciences and Technology (SCTIMST). Although clinical aspects of cases operated upon were reported earlier,[4] a detailed histopathological study was not carried out on them. Preliminary studies indicated the occurrence of mucoid degenerative changes in the aneurysm wall, similar to mucoid vasculopathy, identified by Sandhyamani as a distinct diet induced vascular connective tissue entity in Kerala, resulting from nutritional imbalance with low-protein high-starch diets.[5],[6],[7] A clinico-pathological study was conducted to ascertain the histopathological nature and associated risk factors in cases of cerebral aneurysm admitted to SCTIMST, Trivandrum, during a 2-year period. The observations are presented in this paper.
Material and Methods
During the 2-year period from Jan 1999 to Dec 2000 a total of 255 cases
of cerebral aneurysms were operated on. The present study was conducted
on 57 of these cases where the aneurysm sac could be excised and subjected
to histopathological study. The study did not include mycotic aneurysm.
Aneurysm sacs were fixed in 10% buffered formalin, processed through graded alcohol and embedded in paraffin wax. 5m thick sections were examined, using hematoxylin and eosin, Verhoeff van Gieson′s
and toluidine blue staining techniques. Histopathological observations
were analyzed and correlated with clinical features.
Results
Clinical data
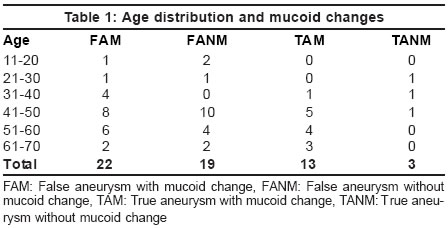
There were 57 patients whose aneurysm sacs were excised during the period Jan 1999-Dec 2000 and were available for analysis. The age of the patients ranged from 17-65 years and there were 33 males and 24 females [Table
- 1]. Twenty-six patients were chronic smokers, 19 patients had hypertension and 3 patients had diabetes mellitus. Of the 23 patients in whom lipid profiles were estimated, 5 had raised total serum cholesterol and 14 had low serum HDL-cholesterol levels. As per the gradation system used by our hospital, 19 cases belonged to the high-income category and 38 cases belonged to the lower income category. Fifty-two patients presented with subarachnoid hemorrhage and 5 patients had no demonstrated subarachnoid bleed. All the patients underwent surgery with clipping of the aneurysms and excision of the sac. Aneurysms involved both anterior (52 cases) and posterior (5 cases) circulation. In selected cases of fusiform aneurysms, the adjoining segment of the affected vessel was also excised. Preoperative angiography had revealed vasospasm in 7 patients. Fifty-four aneurysms were saccular and 3 were fusiform (2 were vertebral artery dissecting aneurysms and 1 was M2 segment aneurysm). Thirty-nine patients were asymptomatic on follow-up, 7 patients had significant residual neurological deficits, 5 patients expired and 6 patients were lost to follow-up.
Histopathology
Histologically, the biopsy samples were classified as: true and false
aneurysms [Table - 2]. The histomorphological features are shown in
[Figure
- 1] and [Figure - 2 a, b, c-d, e]. In 7 false aneurysm cases,
the specimen consisted of extravasated blood clot only, surrounded
at places
by
a thin rim of adventitial fibrous connective tissue. Amongst 50 cases
with an identifiable aneurysm sac, there were 16 true aneurysms and
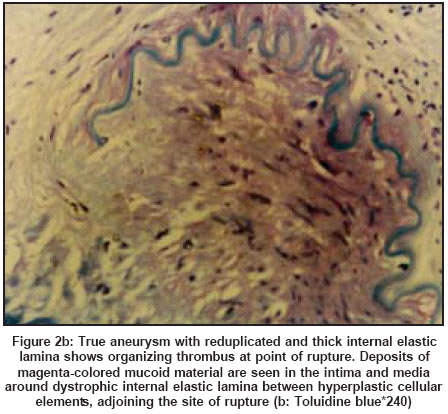
34 false aneurysms. True aneurysms were identified by the presence
of intima, internal elastic lamina and medial elements in the wall,
often with an abrupt or gradual transition to false aneurysm structure,
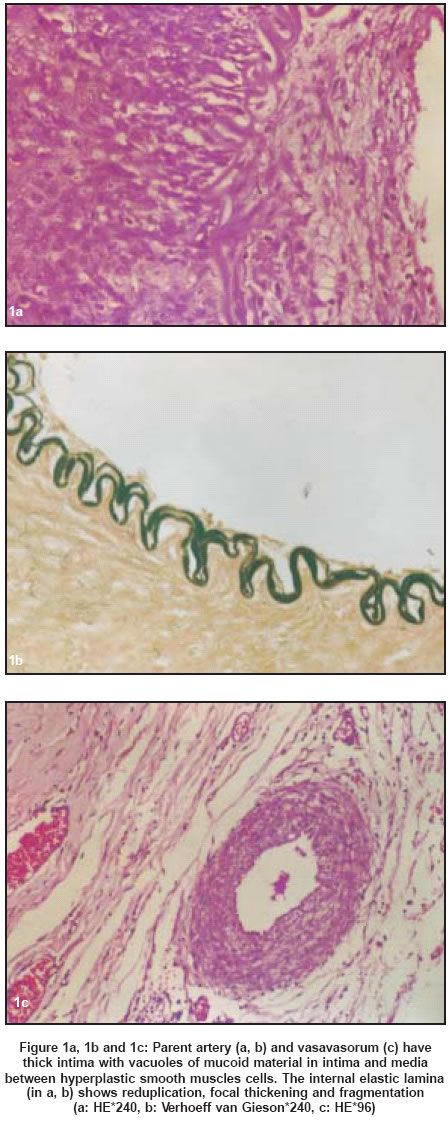
suggestive of focal rupture of the aneurysm sac. The internal elastic
lamina of true aneurysms and of the proximal artery stump where available,
showed varying degenerative changes. It appeared thick and beaded or
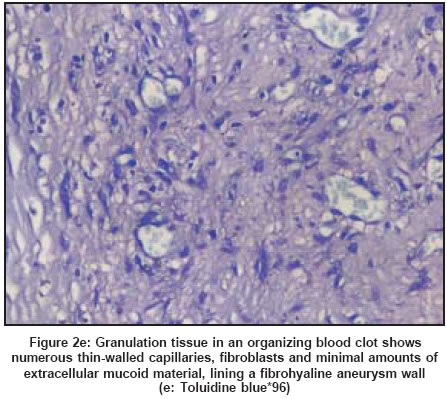
thin attenuated and reduplicated, with focal fragmentation. In false
aneurysms, organizing blood was contained by a fibrous wall, lacking
internal elastic lamina and media, and lined by a layer of thin or
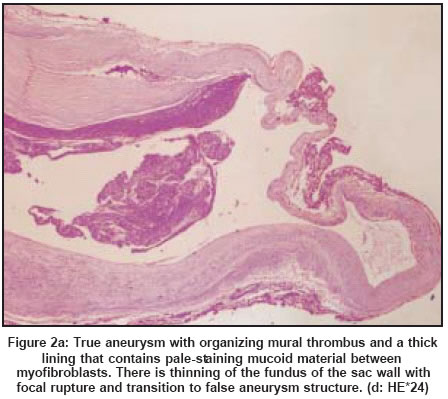
thick exuberant granulation tissue. In 13 true aneurysms and 22 false
aneurysms [Table - 2], the wall had a varying thickness with large
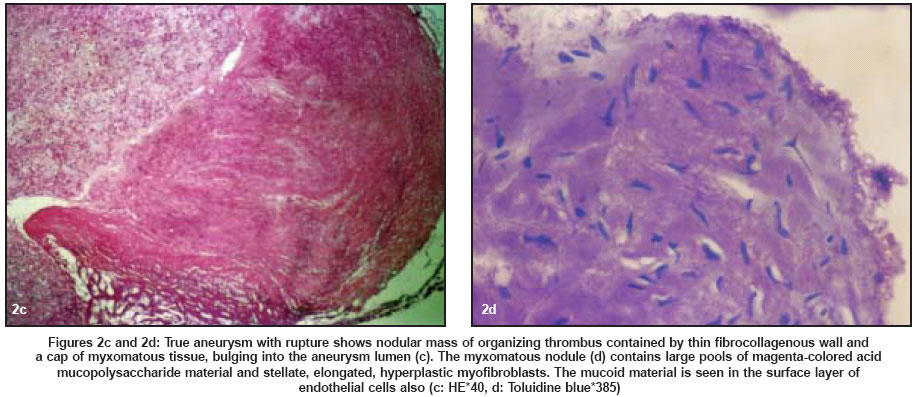
pools of acid mucopolysaccharide material. The mucoid material was
seen between hyperplastic spindle-shaped and stellate myofibroblasts
and in true aneurysms, in the intima and between medial smooth muscle
cells also. In some of the cases, this appeared as mucoid intimal plaques
or nodules of myxomatous tissue bulging into the lumen of the aneurysm.
The proximal artery stump and vasa vasora in some of these cases showed
mucoid degenerative changes in the intima and media. Focal spotty calcification
and hemosiderin deposits were noticed in the aneurysm wall in some
cases. There was no evidence of inflammation and atherosclerosis in
any of the sections of the proximal artery, nor any lipid deposits
(atheromatosis) in the aneurysm sacs.
Clinico-pathological correlation
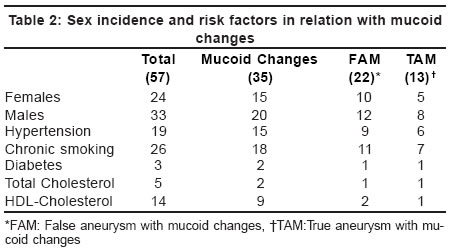
Mucoid changes were commonly seen in patients in the 5th and 6th decades. There were 20 males and 15 females having mucoid changes. Multiple aneurysms with mucoid changes were common in females (4 cases). Middle cerebral artery aneurysms were more common in males (8 cases). Amongst the 35 cases with mucoid changes, 18 patients were chronic smokers, 15 patients were hypertensive, and 2 patients were diabetic, 2 patients had a raised serum total cholesterol level and 9 had a low serum HDL-cholesterol level [Table
- 2]. Ten of the 19 patients in "D" group (high income category of our hospital) had mucoid changes; 12 of the 38 in the lower income groups had mucoid changes. Thirteen of the 16 true aneurysm cases and 22 of the 34 false aneurysm cases showed mucoid degenerative changes and approximately half of the true and false aneurysm cases were associated with risk factors like hypertension and smoking [Table
- 2].
Discussion
In the last decade there was a considerable increase in the number of cerebral aneurysm cases operated upon at this Institute. The number increased from 88 cases in the year 1990 to 136 in the year 2000. Cases of mycotic aneurysm, mostly iatrogenic, following lumbar puncture at peripheral hospitals, were referred to this Institute and reported previously.[1],[2],[3] Besides these, in a large number of cases, the exact nature and cause of the aneurysms were not clear. No infective organisms were demonstrated histologically, nor did the patients have any associated inherited forms of connective tissue disorders. There were no cases with tumour embolism. The present study, carried out on 57 consecutive cases over a period of 2 years, focuses our attention on distinct mucoid degenerative lesions in a number of cases and their association with known risk factors like hypertension and smoking. As reported in the literature aneurysmal rupture is more common in 6th and 7th decades of life,[8] however, in our study group the incidence was more in 5th and 6th decades. In our study the males were predominant, although some studies identify a clear female preponderance (1.6:1).[9] Hypertension has been reported in about 16% to 43.5% of patients with aneurysmal subarachnoid hemorrhage.[10],[11],[12] Hypertension was seen in 33.33% (19) of our cases. Smoking, another important risk factor for cerebral aneurysms[13] was seen in 45.6% (26) of our cases. Although reported occasionally,[14] atherosclerosis is not considered an important risk factor for cerebral aneurysms.[15]
The etiopathogenesis of cerebral aneurysms is uncertain and the cause of subsequent rupture is not evident in all cases.[16] The congenital or medial defect theory hypothesizes a weakness in the artery wall due to maldevelopment.[17] Support
for a congenital origin comes from the frequency of multiple aneurysms,
familial occurrence of aneurysms and association of systemic inherited
diseases of vascular connective tissue, such as Marfan′s syndrome,
Ehlers-Danlos syndrome and inherited forms of dyscollagenosis and polycystic
kidney.[18],[19] Alternately, the degenerative theory suggests an acquired defect in the vessel wall.[20],[21],[22],[23],[24],[25],[26],[27],[28] This theory is supported by the increased frequency of aneurysms with age, hypertension, smoking and arteriosclerosis.[25] The present consensus is that atherosclerosis does not lead directly to the formation of aneurysms.[15],[25] Combinations of maldevelopment and degeneration may also exist. It is known that cerebral arteries differ from extra-cranial vessels in having a thin or absent external elastic lamina. Structural integrity is provided by the internal elastic lamina, the cellular elements dispersed in the extracellular ground substance and fibrillar proteins in the matrix of the intima and media. Any alterations or damage to these vessel wall components, especially the internal elastic lamina and media, along with local hemodynamic factors can lead to the development of aneurysms.[28],[29],[30] The effects of associated risk factors, particularly hypertension and smoking, may be mediated through damage to the internal elastic lamina.[15],[25]
A review of the literature revealed the occurrence of cerebral aneurysms (saccular and dissecting types) with mucoid degeneration, in other parts of the world also, but these were only sporadic reports of single or a small number of cases[27],[29],[31] and therefore not directly comparable with our cases. Various authors used different terminologies such as cystic medial necrosis,[32],[33] intimal fibroelastic thickening,[34] medial mucoid degeneration,[35] segmental mediolytic arteriopathy,[36] myxoid degeneration[27] and mediolytic arteriopathy,[37] to describe the nature of the lesions in the cerebral and extracerebral cervical vasculature. In all these reports, the common finding was the deposition of mucoid material in the intima and media with fragmentation of the internal elastic lamina causing weakening of the vessel wall. Generalized involvement of the extracranial vessels in addition to cerebral vessels has been reported by some.[31],[37] Associated risk factors like hypertension and smoking resulted in further weakening of the wall leading to aneurysm formation, dissection and even rupture.[27]
Mucoid vasculopathy is a non-atherosclerotic, non-inflammatory disorder, with generalized deposition of abnormal acid mucopolysaccharides in the walls of blood vessels, accompanied by dystrophic changes in elastin and collagen.[5],[6],[7] Besides stenotic lesions, the condition was responsible for aneurysms at various sites, such as aorta, pulmonary artery and carotid artery.[38],[39],[40],[41],[42] A monkey model established the role of nutritional imbalance, with low-protein high starch diets, in its etiology.[43] Mucoid vasculopathy is similar to mucoid arteriopathy and aortopathy described from Uganda[44],[45] and to intimo-medial mucoid degeneration described from South Africa[46],[47],[48] where similar diets as consumed in Kerala, may be responsible for mucoid degenerative vascular disease.[49]
In this study, a significant number of patients showed dystrophic changes in the internal elastic lamina. It is well known that structural gaps in the internal elastic lamina are responsible for the development of cerebral aneurysms at bifurcation points.[20] Such gaps aggravated by acquired degenerative changes in elastic laminae may have predisposed arteries to aneurysmal dilatation at bifurcation and non-bifurcation sites in our cases. We postulate that mucoid degeneration and dystrophic changes in the internal elastic lamina in blood vessels are brought about by an acquired disorder of mucopolysaccharide and protein metabolism due to exposure to a low-protein and high-carbohydrate diet for many years. This mucoid and elastic tissue degeneration or mucoid arteriosclerotic vasculopathy, weakens the vessel wall and when combined with risk factors like hypertension and smoking, it may lead to the formation of aneurysms in the 5th and the 6th decades of life. The presence of such histopathological lesions in the parent vessel and in the walls of true and false aneurysms, appears to reflect the underlying diet-induced metabolic disorder and the tendency to lay down excessive amounts of myxomatous tissue during organization of a thrombus or extravasated blood. Estimation of serum mucopolysaccharides was done in a few of our patients and was found to be elevated. This test may be an important marker for the underlying metabolic disorder.
Acknowledgements
The authors are grateful to Dr. K. Mohandas, Director, SCTIMST, Trivandrum, for institutional help; to Dr.V. V. Radhakrishnan, for valuable comments on the histology of five cases and on the paper; to the technical staff of the Department of Pathology and project staff for assistance; and to the Department of Science and Technology, New Delhi, for partial support for carrying out the histopathological studies.
References
| 1. | Radhakrishnan VV, Saraswathy A, Rout D, Mohan PK. Mycotic aneurysms of the intracranial vessels. Ind J Med Res 1994;100:228-31. Back to cited text no. 1 |
| 2. | Rao VRK, Shenoy PT, Pillai SM, Mathews G, Radhakrishnan VV. Cerebral mucormycosis. Neuroradiol 1977;15:291-3. Back to cited text no. 2 |
| 3. | Rao VR, Raman PT, Radhakrishnan VV, Mathews G. Intracranial fungal arteritis. Intracranial fungal arteritis. Ind J Radiol 1980;34:285-93. Back to cited text no. 3 |
| 4. | Rout D. Intracranial sacular aneurysms (Abstract). Presented at 37th Annual Conference of Neurosurgical Society of India, Hyderabad: 1987. pp. 18. Back to cited text no. 4 |
| 5. | Sandhyamani S. Mucoid vasculopathy of unknown etiology. Angiology 1991;42:48-51. Back to cited text no. 5 |
| 6. | Sandhyamani S. Mucoid vasculopathy: vascular lesions in an autopsy study. Mod Pathol 1993;6:333-41. Back to cited text no. 6 |
| 7. | Sandhyamani S, Valiathan MS, Saxena HM. Cardiovascular changes in induced malnutrition. In: SERC Research Highlights, Department of Science and Technology, New Delhi: 1995. pp. 29-36. Back to cited text no. 7 |
| 8. | Pakarinen S. Incidence, aetiology and prognosis of primary subarachnoid hemorrhage: a study based on 589 cases diagnosed in a defined population during a defined period. Acta Neurol Scand 1967;29:1-128. Back to cited text no. 8 |
| 9. | Kassell NF, Torner JCX, Haley EC Jr, Jane JA, Adams HP, Kongable GL. The international cooperative study on the timing of aneurysms surgery. Part I: Overall management results. J Neurosurgery 1990;73:18-36. Back to cited text no. 9 |
| 10. | Bonita R. Cigarette smoking, hypertension and the risk of subarachnoid hemorrhage: a population-based case control study. Stroke 1986;17:831-5. Back to cited text no. 10 |
| 11. | Ostergaard JR, Hog HE. Incidence of multiple intracranial aneurysms. Influence of arterial hypertension and gender. J Neurosurg 1985;63:49-55. Back to cited text no. 11 |
| 12. | Sevet I, Spetzler RF. Intracranial aneurysms and arterial hypertension: A review and hypothesis: Surg Neurol 2000;53:530-42. Back to cited text no. 12 |
| 13. | Adnan I Qureshi, Sung GY, M Fareed K Suri, Straw RN, Guterman LR, L Nelson Hopkins. Factors actors associated with aneurysm size in patients with subarachnoid hemorrhage: Effects of smoking and aneurysm location. Neurosurgery 2000;46:44-50. Back to cited text no. 13 |
| 14. | Shokunbi MT, Vinters HV, Kaufmann JCE. Fusiform intracranial aneurysms. Clinicopathologic features. Surg Neurol 1988;29:263-70. Back to cited text no. 14 |
| 15. | Bryce W, MacDonald R. Intracranial aneurysms and subarachnoid hemorrhage: An over view. Neurosurgery. In: Wilkins RH, Rengachary SS, eds. 2nd edn. McGraw-Hill, New York: 1996. Vol 2. pp. 2197. Back to cited text no. 15 |
| 16. | Weaver JP, Fisher M. Subarachnoid hemorrhage: Update of pathogenesis, diagnosis and management. J Neurol Sci 1994;125:119-31. Back to cited text no. 16 |
| 17. | Forbus WD. On the origin of miliary aneurysms of the superficial cerebral arteries. Bull Johns Hopk Hosp 1930;47:239-84. Back to cited text no. 17 |
| 18. | Schievink WI, Schaid DJ, Rogers HM, Piepgras DG, Michels VV. On the inheritance of intracranial aneurysms. Stroke 1994;25:2028-37. Back to cited text no. 18 |
| 19. | Schievink WI, Parisi JE, Piepgras DG. Familial intracranial aneurysms: an autopsy study. Neurosurgery 1997;41:1247-51. Back to cited text no. 19 |
| 20. | Stehbens WE. Intracranial arterial aneurysms. In: Pathology of the cerebral vessels. Saint Louis: CV Mosby Company; 1972. pp. 351-470. Back to cited text no. 20 |
| 21. | Sheffield EA, Weller RO. Age changes in cerebral artery bifurcations and the pathogenesis of berry aneurysms. J Neurol Sci 1980;46:341-52. Back to cited text no. 21 |
| 22. | Stehbens WE. Histopathology of cerebral aneurysms. Arch Neurol 1963;8:272-85. Back to cited text no. 22 |
| 23. | Yong-Zhong G, van Alphen HA. Pathogenesis and histopathology of saccular aneurysms: review of the literature. Neurol Res 1990;12:249-55. Back to cited text no. 23 |
| 24. | Stehbens WE. Pathology and pathogenesis of intracranial berry aneurysms. Neurol Res 1990;12:29-34. Back to cited text no. 24 |
| 25. | Stehbens WE. Cerebral aneurysms and medial defects, continued. Surg Neurol 2000;53:197. Back to cited text no. 25 |
| 26. | Stehbens WE. Misconceptions of the pathology of intracranial arterial aneurysms. J Clin Pathol 1999;52:708. Back to cited text no. 26 |
| 27. | O'Boynick P, Green D, Batnitzky S, Kepes JJ, Pietak R. Aneurysm of the left middle cerebral artery caused by myxoid degeneration of the vessel wall. Stroke 1994;25:2283-6. Back to cited text no. 27 |
| 28. | Mazutani T, Kojima H. Clinico-pathological features of non-atherosclerotic cerebral arterial trunk aneurysms. Neuropathology 2000;20:91-7. Back to cited text no. 28 |
| 29. | Manz HJ, Luessenhop AJ. Dissecting aneurysm of intracranial vertebral artery: case report and review of literature. J Neurol 1983;230:25-35. Back to cited text no. 29 |
| 30. | Stehbens WE. Apoptosis and matrix vesicles in the genesis of arterial aneurysms of cerebral arteries. Stroke 1998;29:1478-80. Back to cited text no. 30 |
| 31. | Leu HJ. Cerebrovascular accidents resulting from segmental mediolytic arteriopathy of the cerebral arteries in young adults. Cardiovasc Surg 1994;2:350-3. Back to cited text no. 31 |
| 32. | Tse TF, Yu DY. Unusual clinical manifestations of cystic medionecrosis: report of a case. Am Heart J 1972;84:794-800. Back to cited text no. 32 |
| 33. | Bahr M, Postler E, Meyermann R. Fatal stroke in a patient with carotid and middle cerebral artery dissection associated with cystic medial necrosis. J Neurol 1996;243:722-3. Back to cited text no. 33 |
| 34. | Mizutani T, Goldberg HI, Parr J, Harper C, Thompson C. Cerebral dissecting aneurysm and intimal fibroelastic thickening of cerebral arteries. Case report. J Neurosurg 1982;56:571-6. Back to cited text no. 34 |
| 35. | Ide Y, Fukushima T, Yamamoto M, Tomonaga M. Vertebral dissecting aneurysm associated with medial mucoid degeneration. Case report and review of literature. Neurol Med Chir (Tokyo) 1986;26:888-94. Back to cited text no. 35 |
| 36. | Eskarasy-Cottier AC, Leu HJ, Bassetti C, Bogousslavsky J, Regli F, Janzer RC. A case of dissection of intracranial cerebral arteries with segmental mediolytic "arteritis". Clin Neuropathol 1994;13:329-37. Back to cited text no. 36 |
| 37. | Peters M, Bohl J, Thomke F, Kallen K-J, Mahlzahn K, Wandel E, et al. Dissection of the internal carotid artery after chiropractic manipulation of the neck. Neurology 1995;45:2284-6. Back to cited text no. 37 |
| 38. | Ravimandalam K, Rao VRK, Sandhyamani S, Gupta AK, Joseph S, Madhavan Unni M, et al. Focal occlusive disease of the common femoral artery: a case report of 20 cases. Cardiovasc Surg 1994;2:498-502. Back to cited text no. 38 |
| 39. | Waikar HD, Ravimandalam K, Neelakandhan KS, Unnikrishnan M, Sandhyamani S, Mohandas K. Cerebral hyperperfusion syndrome following aortocarotid bypass procedure. J Cardiothorac Vasc Anesth 1993;7:461-5. Back to cited text no. 39 |
| 40. | Gupta AK, Sandhyamani S, Ravimandalam K, Rao VRK, Neelakandhan KS, Joseph S, et al. Multiple pulmonary aneurysms due to mucoid vasculopathy: angiographic and histological observations. Thorac Cardiovasc Surgeon 1993;41:189-92. Back to cited text no. 40 |
| 41. | Waikar HD, Neelakandhan KS, Ravimandalam K, Gupta AK, Sandhyamani S. Case Conference: Case-1-1994. Mistaken diagnosis of coarctation of the aorta with aortoesophageal fistula. J Cardiothorac Vasc Anesth 1994;8:108-13. Back to cited text no. 41 |
| 42. | Neelakandhan KS, Matta R. Extracranial carotid artery aneurysms. Int Angiol 1996;15:316-20. Back to cited text no. 42 |
| 43. | Sandhyamani S. A monkey model for mucoid vasculopathy. Int Angiol 1992;11:256-60. Back to cited text no. 43 |
| 44. | Steiner IO, Hutt MSR. Vascular changes in the idiopathic peripheral gangrene of the tropics. Trop Geogr Med 1972;24:219-25. Back to cited text no. 44 |
| 45. | Steiner I, Thomas JD, Hutt MSR. Aortopathies in Ugandan Africans. J Pathol 1973;109:295-305. Back to cited text no. 45 |
| 46. | Decker GA, Samson ID, Schmaman A. Abdominal aneurysm in South African Negroes due to intimomedial mucoid degeneration. Br J Surg 1977;64:513-6. Back to cited text no. 46 |
| 47. | Cooper K. Extraaortic intimo-medial mucoid degeneration: a clinicopathological study. Angiology 1993;44:477-82. Back to cited text no. 47 |
| 48. | Abdool-Carrim AT, Robbs JV, Kadwa AM, Kenoyer G, Cooper K. Aneurysms due to intimomedial mucoid degeneration. Eur J Vasc Endovasc Surg 1996;11:324-9. Back to cited text no. 48 |
| 49. | Cooper K. Correspondence re: Sandhyamani S. Vascular lesions in an autopsy study (Mod Path 1993; 6:333-341). Mod Pathol 1994;1:715. Back to cited text no. 49 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04020t2.jpg]
[ni04020f2c-d.jpg]
[ni04020f1.jpg]
[ni04020f2a.jpg]
[ni04020t1.jpg]
[ni04020f2e.jpg]
[ni04020f2b.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}