 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
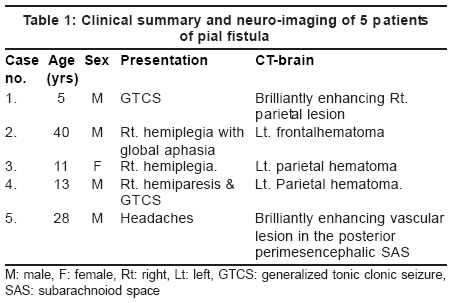
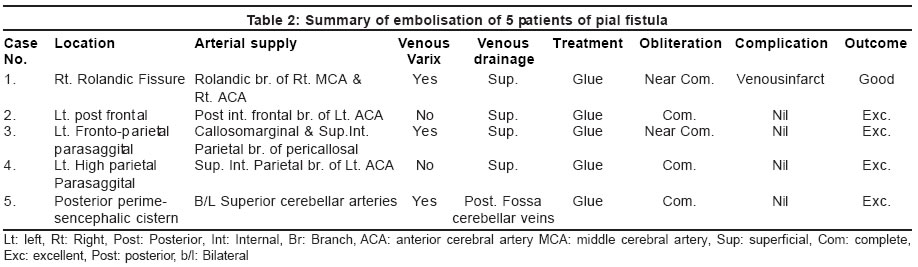
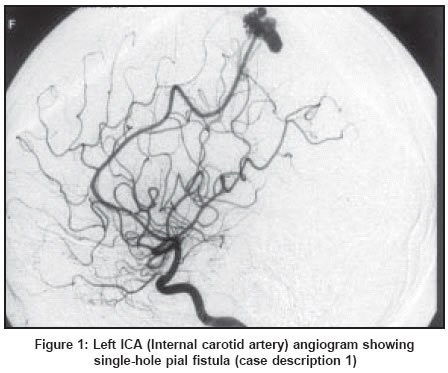
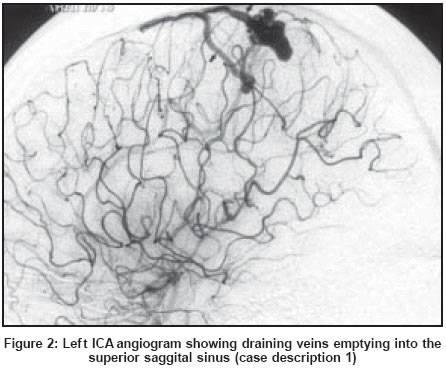
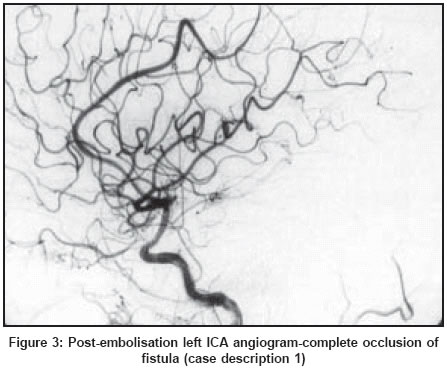
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 87-90 Case Report Endovascular management of intracranial pial arterio-venous fistulas Limaye US, Siddhartha W, Shrivastav M, Anand S, Ghatge S Division of Interventional Neuroradiology, Department of Radiology, Seth G. S. Medical College and King Edward Memorial Hospital, Parel, Mumbai Code Number: ni04021 Abstract From 1996-2002 we treated 5 consecutive cases of pial fistula. There were 3 patients with a single hole-single channel pial fistula and two patients had a complex pial fistula. Three patients presented with intracerebral hematoma and had a focal neurological deficit. One patient presented with history of seizures and 1 patient had headache. The results of the treatment were analyzed both clinically and angiographically. The follow-up period ranged from 6 months to 6 years. All fistulas were treated with concentrated glue. The glue cast included the distal part of the feeding artery, A-V connection and the proximal part of the vein. Post-embolisation angiography showed complete occlusion of two single-hole fistulas and one complex pial A-V fistula and near total occlusion of one single-hole and one complex pial A-V fistula. Four patients had excellent clinical outcome. One patient with single-hole fistula had a hemorrhagic venous infarct resulting in transient hemiparesis.Introduction Intracranial pial arteriovenous fistulas (AVFs) are rare vascular lesions of the brain. They have been recently recognized as distinct vascular anomalies, different from brain arteriovenous malformations (AVMs).[1] These lesions differ from AVMs as they are direct artery to vein connections, have no nidus, and are composed of one or more direct arterial feeders with a single draining vein. Many of these have associated venous varix or giant venous aneurysms.[2],[3] They differ from dural AVFs as they acquire feeders from pial or cortical arteries and are not located within the leaflets of the dura. Intracranial pial fistula is one of the important causes of intracerebral hemorrhage and accounts for 1.6% of all brain vascular malformations.[4] We report 5 cases of pial fistulas treated with glue embolisation via the arterial route. Case Reports From 1996 to 2002, 5 non-traumatic cases of intracranial pial fistulas were treated with Histacryl glue (B.Braun, Tuttlingen, Germany) by the endovascular route [Table - 1] and [Table - 2]. Carotico-cavernous fistulas, vein of Galen malformations and intranidal AVFs in brain AVMs were excluded from this series. Three patients presented with intracerebral hemorrhage and had hemiparesis; 1 patient presented with history of generalized tonic clonic seizures and 1 patient had history of headaches. The intracerebral hematoma was treated conservatively and antiepileptic drugs were used to control seizures.[5],[6] Four of the five pial A-V fistulas were located in the parietal cortex and 1 fistula was located in the perimesencephalic region. Four pial fistulas drained in the superficial venous system and 1 pial fistula drained in the perimesencephalic vein and the pre-cerebellar vein and there was early opacification of the vein of Galen [Table - 1] and [Table - 2]. Treatment was carried out under general anesthesia in all cases. Flow-guided microcatheters were used. Concentrated glue (33%-100%) was used to obliterate the fistulas. During glue injection, blood pressure was maintained at 100mm Hg systolic. All 5 patients were evaluated clinically and angiographically following treatment. These patients were followed up at an interval of 3 months with angiography. Two of the cases are described in detail. Case
1: (Case No 4 in [Table - 1] and
[Table - 2] [Figure
- 1], [Figure
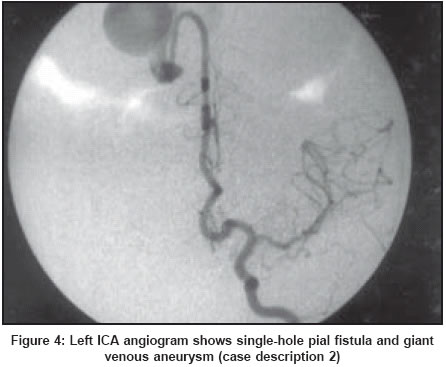
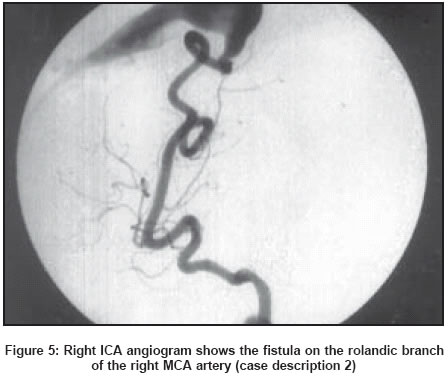
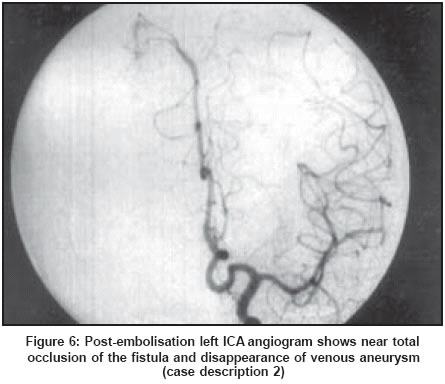
- 2] & [Figure - 3] Case 2: (Case No 1 in [Table - 1]
and [Table - 2] [Figure
- 4], [Figure
- 5] & [Figure - 6] The outcome was evaluated both clinically and angiographically immediately after treatment and at an interval of 3 months. The clinical outcome was graded according to the following scale. Grade 1: Excellent (No deficit, Fully active), Grade 2: Good (Mild deficit, Fully active), Grade 3: Fair (Moderate deficit, Activity impaired), Grade 4: Poor (Severe deficit, Dependent), Grade 5: Dead. Four patients were in Grade 1 and one in Grade 2 [Table - 1] and [Table - 2]. On angiography at 3 months, 2 of the 3 patients with single-hole pial fistula and 1 with complex pial fistula had complete obliteration of the fistula and 1 patient with single-hole and 1 with a complex pial fistula had near complete occlusion. Discussion Pial fistulas are usually congenital arterio-venous brain malformations but can be acquired as in traumatic or iatrogenic cases. Pial fistulas come to clinical attention with intracerebral hemorrhage, seizures, headache, focal neurological deficit and raised intracranial tension. In neonates and infants they may present with high output cardiac failure, increased head circumference and bruit.[5],[6] The natural course of the disease is poor as the risk of hemorrhage is very high. On review of the literature it was seen that 63% of untreated patients succumbed to the disease.[7] Not much is known about the pathophysiology of arterio-venous fistulas. These lesions usually present in childhood, though 2 of the 5 cases in our series presented in adulthood [Table - 1]. Cytokines and vascular growth factors are hypothesized to play a role in abnormal angiogenesis.[8],[9] It is believed that an error in the embryological development of the cerebrovascular tree is responsible for the development of arterio-venous fistulas. A direct communication of the arterial feeder and the single solitary draining vein without any intervening nidus leads to high flow. Due to high pressure and flow transmission, venous aneurysm or giant venous dilatation is seen. During embolisation of high flow fistulas sudden changes in cerebral flow dynamics may occur leading to intracerebral hemorrhage.[10],[11] To prevent this complication the systolic blood pressure was kept at 100mm of Hg during embolisation and for few hours post-embolisation. Pial fistulas can be treated by neurointerventional techniques or by microneurosurgey. Endovascular treatment offers a simple and safe option. Pial fistulas can be occluded with micro coils or Guglemi Detachable Coils, but this usually leads to feeder vessel occlusion and persistent micro A-V connections unless it is a single artery-single vein fistula[12] They may also be occluded with a liquid embolic agent. N- butyl-2 cyanoaccrylate (NBCA) ′Glue′ (B.Braun, Tuttlingen, Germany) is a liquid adhesive embolic agent. It is prepared in different concentrations by mixing it with lipiodol, which also makes it radiopaque. It′s a monomer and polymerizes in contact with an ionic medium. Glue (Histacryl)(B.Braun, Tuttlingen, Germany) was the embolic agent of our choice; concentrated Glue being used in all our 5 cases. It gives fluidity to fill the vascular spaces, control during injection and provides a permanent occlusion. With Glue injection the feeding pial artery can be occluded close to the fistula along with glue penetration into the proximal part of the vein. It is easier to navigate flow-guided microcatheters inside distal cortical cerebral vasculature; over the wire microcatheters, which is essential for use of detachable microcoils. Embolic agents like PVA particles, balloons, coils or silk were not used in this series. The strategy of embolisation depends on the type of fistula treated. In single-channel or single-hole fistula i) single artery -single vein A-V fistula, occluding either the feeding artery, draining vein or the A-V connection, gives the same result. ii) In case of multiple arteries single-hole fistula with single draining venous channel, there is a need to get glue penetrated into the proximal venous channel, distal to the fistula with a continuous glue column. iii) Complex pial fistula[13] (multiple arterial feeders with single venous outlet) was categorized as a fistula in which there are multiple sites of A-V communication, and there are multiple arterial feeders communicating with the draining vein. They are embolised through one of the feeders, preferably the most proximal A-V communication. The portion of the vein with the A-V communication needs to be occluded with Glue. In our series, there was 1 patient with a complex pial fistula where there were multiple arterial feeders draining into a multilobulated venous pouch which later drained into the superior saggital sinus. The patient was treated with concentrated glue and near total occlusion of the fistula was achieved [Table - 2]. Talmonti et al have a similar experience of a complex intracranial A-V fistula.[13] Complex pial fistulas were managed like dural A-V fistulas. In complex pial fistulas the aim is to occlude the draining vein, which has multiple A-V communications. The concept is similar to the occlusion of a dural sinus AVF with transvenous approach and dural sinus occlusion. Careful analysis of the angiogram is essential, because if embolisation is too proximal, new arterial supply recruited or micro A-V connections become macro-connections. In case a normal cortical vein happens to drain into the venous channel of the fistula, it may lead to venous infarction following embolisation. Review of the literature revealed 88 cases of pial AV fistulas reported between 1970-2000. Out of these, 51 patients underwent a direct open neurosurgery and 50 cases were treated with endovascular treatment as an adjunct to surgery or as a primary mode of treatment. Twenty of these 50 cases were unsuccessful.[4] Recent advances in micro-catheter technology allow rapid, safe and more distal intravascular navigation, thus improving the results, safety and reliability of endovascular treatment. As endovascular techniques and technologies progress and the experience of the treating neuro-vascular team grows, the microneurosurgical form of treatment will probably become uncommon. References
Copyright 2004 - Neurology India Free full text also available from: http://www.neurologyindia.com/article.asp?issn=0028-3886;year=2004;volume=52;issue=1;spage=87;epage=90;aulast=Limaye The following images related to this document are available:Photo images[ni04021f2.jpg] [ni04021t1.jpg] [ni04021f6.jpg] [ni04021f5.jpg] [ni04021f1.jpg] [ni04021f3.jpg] [ni04021f4.jpg] [ni04021t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}