 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
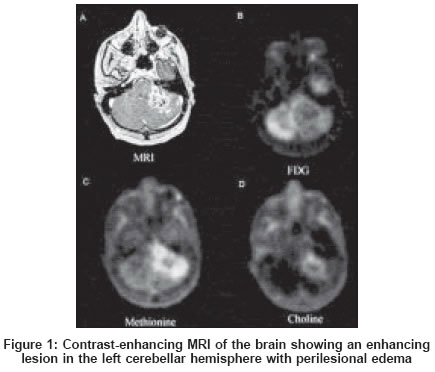
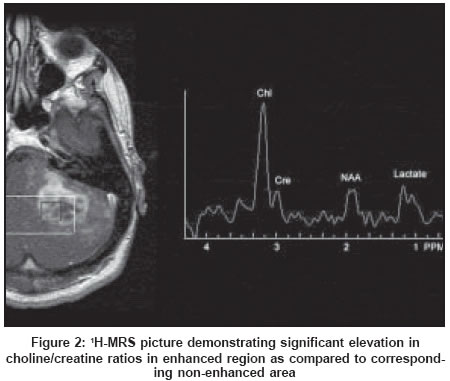
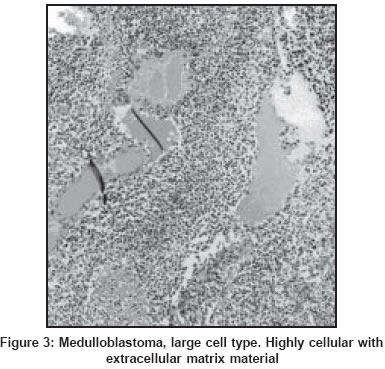
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 91-93 Case Report Radiation-induced medulloblastoma in an adult: A functional imaging study Padma MV, Jacobs M, Kraus G, McDowell P, Satter M, Adineh M, Mantil J Department of Neurology, C. N. Center, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110029 Code Number: ni04022 Abstract We describe functional imaging findings using MRI, 1H-Magnetic resonance spectroscopy and positron emission tomography in a case of radiation-induced medulloblastoma following radiotherapy for pineal gland tumor. MRS showed a prominent choline peak; FDG, 11C-Met and 11C-Choline PET showed a minimal glucose, increased methionine and choline uptake.Introduction Among the adverse effects of radiotherapy, the development of radiation-induced necrosis and induction of a new tumor within the irradiated field has been well described. Although differentiating delayed cerebral radiation necrosis (DCRN) from tumor recurrence is an important clinical question, the distinction cannot be made reliably by conventional imaging techniques. Even with the advances in imaging techniques, occasional cases still pose considerable challenges in interpretation of results and eventual diagnosis. We encountered one such case of radiation-induced medulloblastoma in an adult, following radiotherapy for a pineal gland tumor. The rarity of medulloblastoma in an adult compounded by the fact that it could have been radiation-induced, and the complexity of the functional imaging findings, prompted this case report. Case Report A 29-year-old man was radiologically diagnosed with a pineal gland tumor in 1992 at age 20 and was treated with cranial radiotherapy (wide-field radiotherapy with 3980 centi gray through opposed lateral portals that measured 12 x10.5 cm; there was a cone-down for an additional 540 centi gray in fields that measured 8 x 7 cm). A histological diagnosis of the tumor was never obtained. He remained asymptomatic until December 2000 when he developed diplopia and ataxia. Examination revealed a right third nerve palsy and left cerebellar signs. A contrast enhanced (Gadolinium) MRI of the brain showed a large enhancing mass lesion in the left posterior fossa involving the left cerebellar hemisphere and extending into the vermis, midbrain and pons [Figure - 1]. A diagnosis of a high-grade tumor developing in the field of previous irradiation was entertained. To characterize the lesion further, metabolic screening of the lesion was done with positron emission tomography (PET) scan using 18F-fluorodeoxyglucose (FDG), 11C-methionine (11C-Met), 11C-Choline, and Magnetic Resonance Spectroscopy (MRS). The co-registered MRI and FDG images of the brain demonstrated very minimal to absent glucose uptake in the contrast-enhancing lesion in the posterior fossa. This observation was not suggestive of a high-grade tumor but rather radiation necrosis. The 11C-Met PET study demonstrated areas of increased methionine uptake greater than the cortex in an area corresponding to the contrast-enhancing abnormality noted on the MRI scan. The findings on 11C-Met PET were more suggestive of a tumor, but nevertheless did not exclude the presence of radiation necrosis. 11C-choline PET study suggested the presence of a tumor with prominent 11C-choline uptake, in the region of the contrast-enhancing lesion on MRI. The MRS study showed a large choline peak suggestive of high-grade malignancy, a decreased N-acetyl aspartate peak (NAA) indicative of non-specific neuronal loss, and a mild lactate peak indicative of anaerobic metabolism [Figure - 2]. Cumulative results of MRI, 1HMRS and PET studies therefore, suggested a diagnosis of a dual pathology of DCRN and a radiation-induced tumor. The patient refused therapy and rapidly deteriorated over the next 4 months. An autopsy was performed. The tumor had diffusely infiltrated the left cerebellar hemisphere with extension to the middle and inferior cerebellar peduncles and pons. The tumor was classified as a high-grade medulloblastoma, large cell type [Figure - 3]. Discussion The battery of initial investigations in our patient favored either a dual pathology of DCRN and a radiation-induced tumor or a high-grade tumor alone. DCRN can occur 4 months to 10 years after irradiation, though 70% occur in the first 2 years.[1],[2] The typical appearance of DCRN on structural imaging such as contrast-enhanced CT or Gadolinium-enhanced MRI is a contrast-enhancing mass lesion surrounded by edema and mass effect,[3] which has been seen in the current study. DCRN typically should show hypometabolism on FDG-PET.[4] There is a lack of adequate literature on methionine uptake in radiation necrosis. Low, high and uptake equal to the normal cortex have all been reported.[5],[6],[7] There is no study on choline uptake in radiation necrosis to date. The MRS criteria can differentiate DCRN from tumor.[8] MRS revealed a high choline peak in the present case study, favoring a high-grade tumor over DCRN. Cahan and colleagues first reported criteria to identify whether tumors were induced by radiation treatment.[9] These criteria were fulfilled in the present study. The cumulative actuarial risk of a secondary tumor after cranial irradiation is estimated at 1.7% and 2.5% at 10 and 15 years respectively.[10] Medulloblastoma is the most common posterior fossa tumor in children but accounts for only 1% of all adult brain tumors. Since the histopatholgy of the pineal tumor in our case was never known, it can only be assumed that the medulloblastoma is not a metastatic spread from an original pineal PNET. However, a pinealoblastoma with leptomeningeal spread and metastatic disease developing late after the treatment of the primary is extremely rare in its own right. Limitations in the interpretation of biopsy material, such as sampling error and the heterogeneous nature of the tumor showing variable areas of necrosis, degree of malignancy or even type of cells are well recognized. FDG-PET is sensitive and specific for differentiation of recurrent tumor from radiation necrosis, however, certain limitations remain. Medulloblastomas are reported to be characteristically hypermetabolic. The lack of glucose uptake in the present case is unique and has not been reported earlier. We hypothesize that since the tumor was radiation-induced, this fact may have accounted for de-regulation of the hexokinase activity or alteration of expression of the glucose transporter secondary to the radiation. Therefore, despite a negative FDG-PET in the present study, the presence of a viable high-grade tumor could not be ruled out, especially in view of the 11C-methionine and 11C-choline PET studies and the MRS. This is the first reported case of radiation-induced medulloblastoma in an adult with comprehensive functional imaging analysis. Further studies are required to explain the glucose hypometabolism in radiation-induced medulloblastoma. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04022f2.jpg] [ni04022f3.jpg] [ni04022f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}