 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
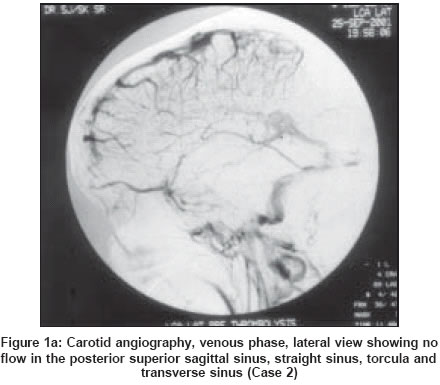
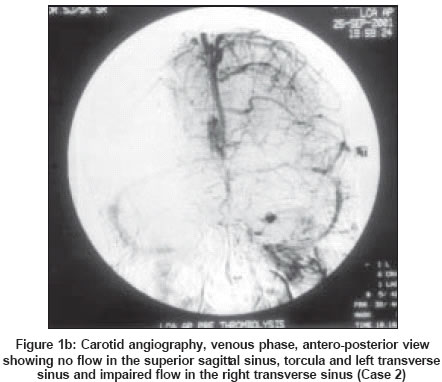
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 96-97 Case Report Blindness, ophthalmoplegia and extensive radiculopathy: An unusual clinical syndrome in intracranial sino-venous thrombosis Moosa A, Kishore A, Gupta AK, Radhakrishnan K Departments of Neurology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum - 695011 Code Number: ni04024 Abstract Isolated intracranial hypertension is a common manifestation of intracranial sino-venous thrombosis (ISVT). Markedly elevated intracranial tension presents with unusual features including cranial neuropathies and radiculopathy. We report two cases with ISVT, which presented with headache, papilledema, progressive visual loss, complete ophthalmoplegia and flaccid areflexic quadriparesis along with a normal sensorium. Magnetic resonance imaging (MRI) of the brain and cervical spinal cord showed no lesions that could account for the neurological deficits. Markedly elevated lumbar CSF pressure was noted in both cases. Nerve conduction study favored radiculopathy in one case and was normal in the other. Raised intracranial pressure was found to be the sole cause for the clinical manifestations. Visual impairment persisted in one patient despite lumbo-peritoneal shunting while the other died of septicemia. To our knowledge there are no previous reports of a syndrome comprising blindness, ophthalmoplegia and flaccid quadriplegia due to intracranial hypertension in ISVT.Introduction Intracranial sino-venous thrombosis (ISVT) has protean clinical manifestations, which include isolated intracranial hypertension, focal neurological symptoms and acute or subacute encephalopathy and a variety of atypical presentations.[1] Various false localizing signs have been reported to occur in patients with raised intracranial pressure (ICP).[2] Radiculopathy as a false localizing sign is extremely rare.[3] We report two cases of ISVT who presented with an unusual syndrome comprising progressive visual loss, ophthalmoplegia and flaccid quadriparesis due to extensive radiculopathy. Raised ICP due to ISVT was found to be the cause for the clinical features. To our knowledge, such a presentation has not been reported in literature till date. Case Report Case 1 Her hematological and basic biochemical parameters were normal. CSF study showed elevated opening pressure with CSF spurting above the 400 mm mark of the manometer. CSF analysis revealed 5 lymphocytes, protein of 0.40 g/L and sugar of 0.50 g/L. Digital subtraction angiography (DSA) showed thrombosis in the posterior superior sagittal sinus, torcula and right transverse sinus. Urine homocysteine, anti-nuclear antibody, anti-phospholipid antibody and sickling test were negative. Visual evoked potential to strobe stimulation showed major positivity at 187 ms in the right eye and was inelicitable in the left eye. The nerve conduction study including F-waves, was normal. She underwent a lumbo-peritoneal shunt following which her ophthalmoplegia and limb weakness improved over two weeks. She was continued on anticoagulants. At one-year follow-up, she had bilateral optic atrophy and only a marginal improvement in vision. Case 2 At admission she was hemodynamically stable and had a normal sensorium. She had bilateral severe papilledema with fundal hemorrhages. She had no light perception in either eye. Complete external and internal ophthalmoplegia without ptosis and facial diplegia was noted. Motor examination revealed generalized hypotonia and areflexia with Grade 2 power of proximal limb muscles, trunk and neck, and Grade 3+ power of distal muscles. No sensory impairment was found. She had moderate neck stiffness and Kernig′s sign was positive. Laboratory investigations revealed mild leukocytosis. Her routine biochemical parameters were normal. MRI brain showed a small left parietal hemorrhagic infarct and evidence of superior sagittal sinus thrombosis. DSA showed thrombosis of the superior and inferior sagittal sinuses, straight sinus, torcula and right transverse sinus [Figure:1a] and [Figure:1b]. The prothrombin time, partial thromboplastin time, serum homocysteine level, protein S and C activity, and anti-thrombin III activity were all in the normal range. Anti-cardiolipin antibody, anti-phospholipid antibody, anti-nuclear antibody, rheumatoid factor, tests for sickling and factor V Leiden mutation and work-up for myeloproliferative disorders were negative. Nerve conduction study showed inelicitable F-waves in all four limbs; other conduction parameters were normal. Sinus patency was achieved with dural sinus thrombolysis with urokinase. This led to improvement in the limb power while other deficits remained the same. Two days later she developed dense quadriplegia with respiratory muscle weakness requiring mechanical ventilation. Her sensorium remained clear and she had no long tract signs. MRI brain and cervical spine were repeated which showed no additional infarcts. MRV showed re-thrombosis of sinuses; repeated thrombolysis failed to achieve sustained sinus patency. In view of visual loss secondary to papilledema, lumbar CSF pressure was measured and found to be more than 850 mm of CSF. CSF analysis showed 2 lymphocytes, protein of 0.44 g/L and sugar of 0.56 g/L. In view of visual loss secondary to intracranial hypertension, lumbo-peritoneal shunting was performed. Immediately following shunting her pupils reduced in size, reacting briskly to light along with a mild improvement in external ophthalmoplegia and handgrip. A repeat lumbar puncture 3 days after surgery showed normal CSF pressure of 180 mm. A repeat nerve conduction study showed appearance of F-waves in the right upper limb; other parameters remained unchanged. However, in the ensuing days she developed fulminant Klebsiella septicemia and died. Consent for autopsy was refused. Discussion The two cases of angiographically proven ISVT reported here had remarkably similar clinical features, consisting of acute bilateral visual loss, complete internal and external ophthalmoplegia, areflexic flaccid quadriparesis and normal sensorium along with raised ICP. MRI brain and spine showed no abnormalities that could directly account for the deficits. Reduction in CSF pressure was associated with partial recovery suggesting a possible role of intracranial hypertension in the pathogenesis. Though blindness and ophthalmoplegia are well-known manifestations of raised ICP, flaccid quadriparesis is extremely rare.[2] We initially considered the possibility of midbrain infarction secondary to deep cerebral venous thrombosis as the cause for areflexic quadriparesis with ophthalmoplegia. However, MRI brain, done twice in the second case, showed no lesion in the brainstem. Cavernous sinus thrombosis was excluded on angiography. Various cranial nerve palsies due to raised ICP are well described in the literature.[2] This has been attributed to a direct effect of raised ICP causing distortion or displacement of brainstem structures and or cranial nerves.[2] Kuehnen et al described cases of transverse and sigmoid sinus thrombosis presenting with isolated cranial nerve palsies, presumably due to thrombosis of pontine and medullary veins.[4] But the prompt reversal of oculomotor paralysis in our first case and immediate recovery of pupillary paralysis after the lumbo-peritoneal shunt in our second case favors raised ICP as the cause of oculomotor palsy. With a normal MRI of brain and spinal cord, flaccid areflexic quadriplegia in our cases is likely to be due to a lower motor neuron involvement. The inelicitable F-waves with normal peripheral conduction study in our second case supported a radicular involvement.[5] Needle electromyography could not be performed as our patients were on anticoagulants. The normal nerve conduction study in the first case could be due to milder involvement and dilution factor.[5] Minor manifestations of radiculopathy in the form of acral paraesthesias[6] and spinal and radicular pain have been described in patients with pseudotumour cerebri.[7],[8],[9] Recently, Obeid et al reported two patients with extensive radiculopathy due to intracranial hypertension; one patient had pseudotumour cerebri and the other ISVT.[3] Both had papilledema and impending visual loss. Electrodiagnostic study showed features of a diffuse radiculopathy. Both cases were diagnosed initially as Guillain-Barre syndrome (GBS) and were treated with intravenous immunoglobulin without benefit. They responded well to lumbo-peritoneal shunt supporting the view that raised ICP was responsible for the radiculopathy. However, unlike our cases, ophthalmoplegia was absent in these cases. Ophthalmoplegia with quadriplegia as seen in our cases may resemble Miller Fisher- Guillain- Barre overlap syndrome clinically. However our cases had normal CSF protein and nerve conduction study was not diagnostic of GBS in either of them. Longstanding radiculopathy can lead to axonal loss and simulate axonal forms of GBS electro-physiologically also.[3] Though it is well known that papilledema rarely does occur in GBS, cases with atypical or normal electrophysiological study should be viewed with suspicion; CSF pressure testing and MRV or DSA would be advisable to exclude ISVT in such cases. We suspect that the mechanism of radicular dysfunction is due to elevated CSF pressure distending the subarachnoid space around the nerve roots resulting in mechanical stretching and pressure effect. Enlargement of the spinal subarachnoid space along with distended root pouches has been reported in a patient with radiculopathy due to idiopathic intracranial hypertension.[7] Venous ischemia of nerve roots secondary to impaired venous outflow through the thin-walled radicular veins may also play a role.[10] Motor roots appear to be more vulnerable as weakness was the major deficit in our cases and in those reported by Obeid.[5] We propose that a marked rise in ICP produces a potentially reversible dysfunction of the cranial nerves and spinal nerve roots leading to this unusual clinical syndrome. In our experience, such cases appear to be at risk of irreversible visual loss. In conclusion, we report that the syndrome of visual impairment, ophthalmoplegia and flaccid quadriparesis in patients with ISVT signifies a markedly raised ICP. Hence, patients with these manifestations should be treated early and aggressively to decrease the ICP to safe levels. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04024f1a.jpg] [ni04024f1b.jpg] |
| |||||||||

{kind=link}
{kind=link}