 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
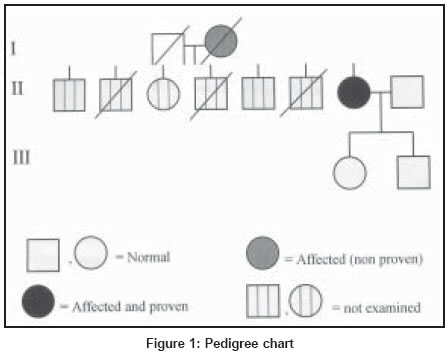
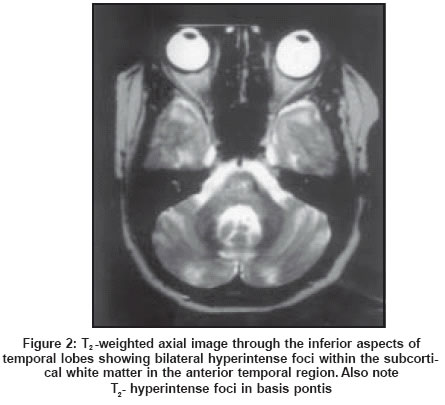
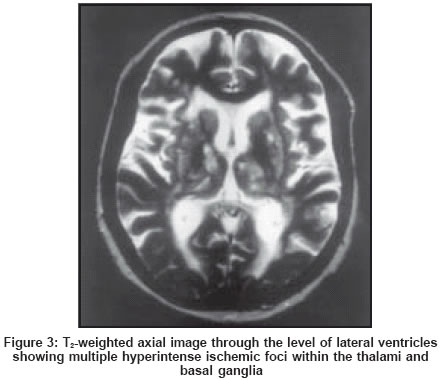
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 99-101 Case Report Cerebral autosomal dominant arteriopathy with subcortical infarcts and leucoencephalopathy (CADASIL): A case report with review of literature Gurumukhani JK, Ursekar M, Singhal BS Bombay Hospital Institute of Medical Sciences, 12, New Marine Lines, Mumbai - 400020 Code Number: ni04025 Abstract Cerebral autosomal dominant arteriopathy with subcortical infarcts and leucoencephalopathy (CADASIL) is an inherited arterial disease, commonly overlooked or misdiagnosed. We report a case of CADASIL in a 51 years old woman who presented with progressive subcortical dementia, recurrent ischemic events and seizures in the absence of known vascular risk factors of five years’ duration. Her mother had a history of similar illness. Magnetic resonance imaging (MRI) of brain revealed subcortical and deep white matter hyperintense lesions within the cerebral white matter on T2-weighted images. DNA mutation of Notch 3 gene confirmed the diagnosis of CADASIL. Introduction Tournier-Lasserve et al first introduced the acronym CADASIL (cerebral autosomal dominant arteriopathy with subcortical infarcts and leucoencephalopathy) in 1993 and mapped the gene locus to chromosome 19q12.[1] This disease with autosomal dominant inheritance is characterised by subcortical ischemic events, vascular dementia, and migraine with aura and mood disorders. We report a genetically confirmed case of CADASIL which has not been reported previously from India. Case Report A 51-year-old woman presented with the complaints of difficulty in walking (5 years), forgetfulness (4 years), dysarthria (2 years), and incontinence (2 years) in January 2001. In 1997 she had weakness of both lower limbs (left more than right). Her MRI of cervical and dorsal spine and cerebrospinal fluid examination including IgG was normal. Three months later she became mildly forgetful. MRI brain done at this time revealed multiple, hyperintense periventricular white matter lesions on T2-weighted images. She had no vascular risk factors such as hypertension, diabetes or dyslipidemia. Carotid doppler studies, visual and brainstem evoked potentials were normal. Considering demyelination as a possibility she was given intravenous methylprednisolone. Her condition continued to worsen; she needed support to walk, speech became dysarthric, she developed occasional incontinence, left lower motor neurone facial palsy, and diplopia. When we saw her in January 2001 she denied history of any significant headaches. On examination the patient cooperated and had a score of 18/30 mini-mental testing. She had spastic dysarthria. External ocular movements were full without nystagmus. Other cranial nerves and fundi were normal. She had mild spastic weakness in all four limbs with brisk tendon jerks and extensor plantars. There was no sensory deficit or cerebellar signs. Examination of other systems was normal. The pedigree chart is shown in [Figure - 1]. Her mother had a similar progressive illness of three years duration with difficulty in walking, dysarthria, cognitive impairment, and incontinence with white matter changes in brain MRI. The patient′s routine blood examination, chest x-ray and ECG were normal. Her repeat brain MRI revealed confluent and discrete, fairly symmetric T2 hyperintense foci in the deep and subcortical white matter of the cerebral hemispheres. Similar foci were present in the brainstem, thalami, basal ganglia and the subcortical white matter of anterior temporal lobes. [Figure - 2] and [Figure - 3]. These changes were more extensive compared to the MRI in 1997. Considering the possibility of CADASIL, genetic studies were done by by sequencing exons 3 and 4 of the Notch 3 gene. It showed substitution of a nucleotide at position 499 (codon CGC was transformed to TGC ) in exon 4. This resulted in the replacement of an arginin by a cystein at position 141 in the 3rd EGF motif. This type of mutation was observed only in CADASIL patients and not in a panel of 200 control chromosomes in the laboratory of Tournier-Lasserve. Few weeks later she had two generalized seizures. Her condition continued to worsen, she became bed bound and died at home at the age of 52 years. Discussion CADASIL often starts with attacks of migraine with aura during the third decade followed by ischemic events around 10 years later, dementia approximately 20 years after onset and death during the sixth decade. Most of the ischemic events, transient or permanent, are classic lacunar infarcts that arise in the absence of hypertension or any other recognised vascular risk factors. Chabriat et al described 45 family members (23 males and 22 females) belonging to seven families.[2] They observed subcortical ischemic events in 84%, progressive or stepwise subcortical dementia with pseudobulbar palsy in 31%, migraine with aura in 22% and mood disorders with severe depressive episodes in 20%. Although Chabriat et al did not report seizures in any of his patients, Dichgans et al in his series of 102 CADASIL patients noted seizures in 10 patients.[3] MRI findings in CADASIL include symmetrical and extensive hyperintense signal within the cerebral white matter on T2-weighted images and well defined hypointense lesions on T1- weighted images, suggestive of infarcts within the deep white matter and basal ganglia. Such multiple focal lesions are also seen in ischemic leukoaraiosis. O′sullivan et al found hyperintensities in white matter of anterior temporal lobe to be highly sensitive (90%) and specific (100%) for CADASIL.[4] Involvement of external capsule, though less specific, was seen early in the disease course, and in few patients involvement of corpus callosum was observed. The likely explanation for the selective involvement of the anterior temporal white matter and external capsular areas in CADASIL as opposed to ischemic leukoariosis is that the process involves slightly larger leptomeningeal vessels. There is pathologic evidence to support the involvement of large leptomeningeal vessels in CADASIL, which are often spared in ischemic leukoariosis.[5] The pathological hallmark of CADASIL is a non-amyloid, non-atherosclerotic microangiopathy.[6],[7] The vasculopathy generally affects the leptomeningeal and perforating arteries of the brain between 100-400 mm in diameter. The media of these vessels is thickened by eosinophilic periodic-acid-Schiff positive granular deposits. On electron microscopy, this material corresponds to osmiophilic immunoglobulin-like deposits located in close proximity to vascular smooth muscle cells.[7] CADASIL is an inherited disease with mutations in the transmembrane receptor of the Notch 3 gene on chromosome 19q12.[8] Notch 3 is a 2321 aminoacid type I transmembrane protein, which is believed to be involved in the specification of cell fate during development.[9] Joutel et al screened for mutations in the 33 coding exons of the Notch 3 gene in 50 patients suspected to have CADASIL and observed mutations in 45/50 (90%) patients.[8] A striking feature was that of the 45 patients having mutations, 32 had mutations restricted to exon 3 or 4. The authors therefore suggested that screening for mutations in the Notch 3 gene could be used as a diagnostic test for CADASIL. The test would involve two steps: initial screening of exons 3 and 4, and only if no mutations were present, would the remaining 31 exons be analysed. Our patient was found to have mutation in the exon 4 of notch 3 gene, thus confirming the diagnosis of CADASIL. The disease is probably underdiagnosed. The diagnosis should be considered not only in patients with recurrent small subcortical infarcts leading to dementia, but also in the patients with transient ischemic attacks, migraine with aura and mood disturbances, whenever MRI reveals prominent signal abnormalities in the subcortical white matter and basal ganglia. Acknowledgements We are grateful to Prof. Marie-Germaine Bousser for her comments on the history of the patient and MRI images and We thank Prof. E. Tournier-Lasserve and Dr. A. Joutel (Laboratory of genetics, Lariboisière, Paris) for conducting the genetic study. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04025f3.jpg] [ni04025f1.jpg] [ni04025f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}