 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
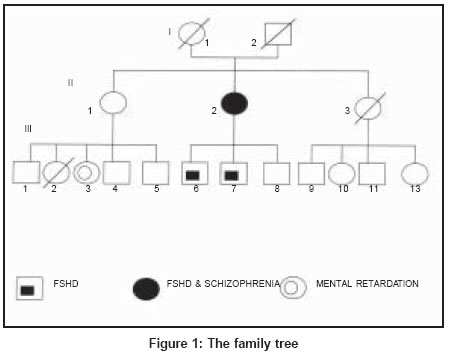
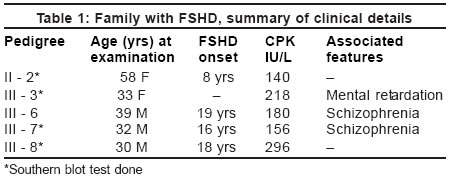
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 104-105 Case Report Association of schizophrenia and mental retardation with facio-scapulohumeral muscular dystrophy Sharma S, Namrata S Department of Neurology, MMI Hospital, Lalpur, Raipur (C.G.) - 492007 Code Number: ni04027 Abstract Three members of an Indian family with facio scapulohumeral dystrophy (FSHD linked to chromosome 4q35 with short EcoR1 segment of 23 Kb are reported where two male adults had schizophrenia. One family member developed isolated facial weakness with mild mental retardation. This genetically proven FSHD family is reported because of its uncommon associations.Introduction Facio scapulohumeral dystrophy (FSHD) is an autosomal dominant muscle disease, usually presenting before the age of 20 years. FSHD results from a deletion of integral copies of a 3.3 Kb DNA repeat motif named D4Z4 on chromosome 4.[1],[2] Association of schizophrenia with FSHD is unknown. The current hypothesis for causation of schizophrenia involves multiple genes with mild to moderate effect and non-genetic risk factors.[3] The mental retardation is a described feature of childhood FSHD with larger deletion defect.[4],[5] An Indian FSHD family is reported where two male adults had schizophrenia and one additional family member had isolated facial weakness and mild mental retardation. FSHD has been linked to 4q35 with short EcoR1 segment of 23 Kb in these three patients. It is suggested that schizophrenia may be an association of FSHD. Case Report The family pedigree [Figure - 1] based on information available of 17 family members in three generations indicates that the pattern of inheritance is autosomal dominant. Family members with FSHD were evaluated in detail and DNA studies were performed. The mother in the described family (II-2), a 58-year-old woman developed muscle disease at the age of 8 years. She had advanced disease-involving face with inability to close eyes, hollowed cheeks with persistent pouting, markedly wasted shoulder girdle and brachial muscles, abdominal muscle weakness and exaggerated lumbar lordosis. The deep tendon reflexes were absent. She was self-dependent for activities of daily living. All her three sons developed FSHD. The disease was confined to wasting and weakness of face, shoulder girdle and upper extremities. The deltoid and forearm muscle mass was relatively preserved. The deep tendon reflexes were absent in the upper limbs. The elder two of them became schizophrenic in addition at the age of 30 and 15 years. The estimation of serum CPK done in all the cases was near the normal range. The needle EMG revealed a myopathic pattern with reduced duration and amplitude of the motor potential, increased polyphasic potential, more marked in the brachial biceps. The muscle biopsy done in two patients showed marked variation in fiber size, some of the fibers were small atrophic, while some were large hypertrophied. There were foci of interstitial mononuclear infiltrates, consistent with the diagnosis of FSHD. The Southern blotting analysis performed using p13 E-11 probe in family members confirmed 4q35-linked FSHD. All three patients had short EcoR1 fragment of 26 Kb that became shortened to 23 Kb by EcoR1/B1n1 double digestion. One other family member (III-3) had facial weakness without shoulder girdle and upper limb involvement. She also had mild mental retardation with IQ of 75. The DNA analysis revealed an EcoR1 fragment of the same size [Table - 1] Discussion FSHD is characterized by progressive weakness of the muscles of the face, upper arms and shoulder girdle. Early onset FSHD is often associated with retinal telangiectasia and sensorineural deafness.[6] Genetic linkage has mapped the FSHD gene to the subtelomeric region of chromosome 4q35. Detection is done by Southern blot analysis of DNA using the p13E-11 probe. An ECOR1 fragment less than 38 Kb is associated with FSHD. The shorter fragment length produces more severe and early manifestation of the disease.[7],[8] Recently, six sporadic cases with atypical presentation like facial-sparing disease and lower limb involvement at the onset have been described and confirmed on DNA testing, however parental genetic tests have not been performed.[9] The present FSHD family had short EcoR1 segment of 23 Kb. To the best of our knowledge this is first Indian family reported with genetic studies. Early onset FSHD with severe mental retardation and epilepsy has been described from Japan.[4] Funakoshi et al (1990) reported a high frequency of both mental retardation and epilepsy with smallest ECOR1 fragment of 10-11 Kb. One of our family members had mild mental retardation and isolated facial weakness with ECOR1 fragment of 23 Kb. A number of specific genes like the 5 - hydroxytryptamine type 2-a receptor gene, dopamine D3 receptor gene localized to multiple chromosomes including 6p, 6q, 8p, 13q and 22q are suggested to be involved in the causation of schizophrenia.[3] It is not a described feature of FSHD. Zatz et al reported a family in which four of five adult patients with Becker muscular dystrophy had schizophrenia or related spectrum. They postulated the possible locus for schizophrenia on XP-21 or a possibility of an abnormal expression of the dystrophy gene itself. This case report suggests that FSHD can have uncommon central nervous system involvement and should be specifically evaluated in Indian FSHD families. Acknowledgements The authors wish to thank Yukiko K.Hayashi, M.D, Kanako Goto, Department of Neuromuscular Research, National Institute of Neuroscience, NCNP, Kodaira, Tokyo, Japan for performing the Southern blot analysis of our patients. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04027f1.jpg] [ni04027t1.jpg] |
| |||||||||

{kind=link}
{kind=link}