 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
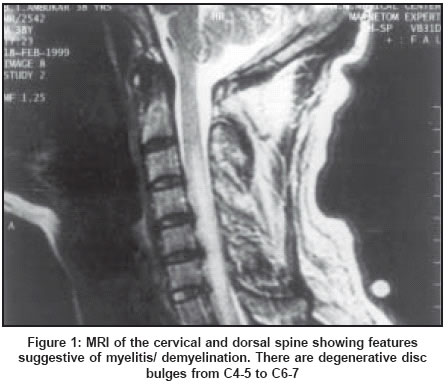
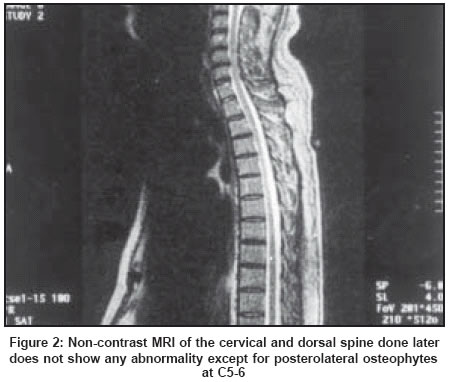
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 106-108 Case Report Biphasic demyelination of the nervous system following anti-rabies vaccination Kulkarni V, Nadgir D, Tapiawala S, Malabari A, Kalgikar A, Kela R, Nadkar M, Kamath S, Shah A Department of Medicine and Neurology, TN Medical College & BYL Nair Charitable Hospital, Mumbai - 400 008 Code Number: ni04028 Abstract Acute Disseminated Encephalomyelitis (ADEM) is an acute or subacute condition characterized by widespread multifocal neurological deficits of variable severity. We report a case of a 45-year-old man with ADEM following Anti-Rabies vaccine (ARV). Introduction ADEM can occur following vaccination against rabies, small pox and rarely after tetanus antitoxin. Exanthematous diseases, infectious diseases and neoplasia are other etiological factors. The incidence with suckling mouse brain vaccine is 1 in 7865 vaccinations whereas it is 1 in 25,000 with duck embryo vaccine.[1] Case Report A 45-year-old male presented with complaint of retention of urine, paraesthesia and weakness in all four limbs in all the muscle groups for one day. The patient had suffered a dog bite 14 days prior to admission and he had taken anti-rabies vaccine [Rabies Vaccine Human (Neural tissue) IP BPL Inactivated - Sheep brain suspension 5% w/v, Antigenic value > 0.3] for 9 days. Neurological examination revealed normal higher functions. Motor system examination revealed that power was 4/5 in both upper limbs and 3/5 in both lower limbs. There was generalized hypotonia. Right corneal reflex was depressed and sensations on the right half of the face were reduced by 50%. The sensations for all the modalities were decreased below T2 dermatome level. Reflexes were bilaterally hyperactive with the left-sided being more brisk than the right-sided. Plantars were extensors bilaterally. Cerebellar signs were elicited on the left side of the body and he had cerebellar ataxia. CSF examination showed lymphocytic pleocytosis (21 lymphocytes per cmm) with normal sugar (60-mg%) and proteins (15-mg%). MRI of cervical and dorsal spine showed a long segment intramedullary hypointense signal on T1 weighted images extending from C3 to D9 levels which became hyperintense on T2 weighted images. These features were suggestive of myelitis/ demyelination [Figure - 1]. MRI brain was normal. In view of demyelinating disease the patient was treated with injection methyl prednisolone 1 gm intravenously for 3 days followed by oral tablet prednisolone. The patient improved in motor weakness and was discharged with almost normal power, on tapering doses of oral steroids. He had a residual sphincter disturbance for which he was taught self-intermittent catheterization. After about a month the patient complained of blurring of vision in the left eye. Acuity of vision in the left eye was 6/12. There was afferent pupillary defect in the left eye with normal fundus examination bilaterally. CSF examination for oligoclonal bands was negative. MRI of cervicodorsal spine [Figure - 2] and brain with optic nerve cuts did not show any abnormality. His visual evoked potentials (VEP) showed prolonged P100 latencies from both eyes suggestive of bilateral optic neuritis. The diagnosis of Neuromyelitis optica was considered in view of myelitis and bilateral optic neuritis. The patient was given intravenous methyl prednisolone pulse for three days followed by oral steroids in tapering doses. He made a complete clinical recovery with normal visual acuity. Patient′s further follow-up as yet has not shown any relapse. Discussion Acute disseminated encephalomyelitis (ADEM) is, indeed, the most common demyelinating disease in the world because of the frequency with which it follows measles and other viral infections.[2] It has been described after a number of immunizations, particularly small pox and rabies.[3] In recent years, several reports of new cases of CNS demyelination or reactivation of multiple sclerosis after hepatitis B vaccination have raised a possibility of a causal link.[4],[5] ADEM is an immune-mediated disease. It is characterized by early destruction of myelin due to structural homology between the brain tissue and myelin proteins and the brain-derived tissue in ARV. The incidence of ADEM following neural anti-rabies vaccine is 1/300 to 1/7000 as compared to 1/50,000 following non-neural vaccine.[3],[6],[7] The reactions are less when less than 7 injections are taken whereas they are more after 14 injections.[8] Patholologically, ADEM is characterized by perivenous inflammation and demyelination in the CNS. Antibodies cross-react with brain tissue to give perivenous inflammation, multifocal meningeal infiltration, demyelinating foci and destruction of nervous tissue.[3],[9] ADEM is classically differentiated from multiple sclerosis (MS) by the intensity of inflammation.[9],[10] The highest density of cells is at the edge of the perivenous lesions in MS whereas it is at the center of the lesion in ADEM.[1] Although ADEM is a white matter process, lesions can be found in the gray matter also. Involvement of gray matter is possible in MS as well.[1],[9] ADEM often produces a widespread CNS disturbance with coma or drowsiness, seizures and multifocal neurological signs implicating the cerebral hemispheres, cerebellum, brainstem, spinal cord and optic nerves. In contrast, MS usually presents as a monosymptomatic syndrome such as optic neuritis or a subacute myelopathy. Thus optic neuritis in ADEM is usually simultaneously bilateral whereas in MS it is more often unilateral; myelopathy in MS is frequently partial but in ADEM it is often complete and associated with areflexia. Fever and meningism which are characteristic of ADEM, are virtually never present in MS.[10] Our patient was afebrile and had no signs of meningism. A moderate pleocytosis is usual in ADEM, high cell count may occasionally be seen in MS; and although oligoclonal IgG bands are a characteristic feature of MS, they may also occur in ADEM.[10] MRI is the imaging modality of choice for demonstrating the lesions of demyelinating diseases.[9],[11] Bilateral symmetric involvement in the parieto-occipital white matter, cereballar peduncles and white matter and deep gray matter are more suggestive of ADEM.[10] Discrete multiple lesions and symmetric lesions of the internal capsule and thalamic involvement are unlikely to be the features of MS.[1] These aspects do not have an absolute diagnostic value, as up to 25% of patients with MS may exhibit basal ganglia lesions.[12] In MS, lesions would be of varying age; in most patients with ADEM, they would all be the same age. Given that ADEM is usually a monophasic disease, it might be expected that all lesions would enhance in the acute phase, while none would do so in the chronic phase.[10],[13] However, in ADEM the appearance of new lesions remains possible, generally within a few weeks after acute presentation, with a coincident progression of clinical symptoms.[9] Lesions may persist for a long time after acute presentation despite clinical improvement.[10],[13] It is even more difficult to differentiate MS from ADEM when neurological disturbances recur after a pseudo-typical presentation of ADEM up to 18 months after the initial presentation. In such cases a minimum period of 6 months is required between two episodes for them to be considered as relapses of MS.[10] MS is by definition a multiphasic disease which frequently results in stepwise or steady progressive deterioration in neurological function. ADEM also may not be as monophasic as previously described.[2],[14] To distinguish ADEM from a first attack of MS is often difficult. So a long follow-up is required. S. Schwarz concluded that many patients initially diagnosed with ADEM develop clinically definite MS upon long-term follow-up.[15] With many similarities in clinical presentation, MR findings and putative pathogenesis, it appears reasonable to consider ADEM as part of the spectrum of inflammatory demyelinating diseases.[16] In most patients ADEM is monophasic lasting from 2 to 4 weeks. However, recurrent attacks have been reported.[17] Slight motor weakness, sensory disturbances, ataxia and difficulty with bladder control may remain, especially following dorsolumbar myelitis.[18] Steroids were found to be helpful in an uncontrolled study.[19] Our patient had bilaterally abnormal visual evoked potential responses during his second admission. Hence, the diagnosis of Neuromyelitis optica, a variant of MS should be considered in this case. In the classical presentation there is involvement of both optic nerves and the spinal cord, evolving over a few days or weeks; initial manifestation may be at the either site.[20] The frequency of this type of presentation is seen to be higher in Japan and in tropical countries like India.[21],[22] It is usually a monophasic illness, although sometimes there is a relapse of spinal cord dysfunction or optic neuritis or the appearance of a lesion at a new site, suggesting that it is a variant of MS. This patient had presented as a case of ADEM following anti-rabies vaccination but subsequently developed bilateral optic neuritis. There is a possibility that it may be MS activated by ARV. But further follow-up of the patient as yet has not shown any relapse. There have been, however, reports of MS being triggered off by mild infection or immunization.[23] There is no report in the literature of any such case evolving into MS.[1] References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04028f1.jpg] [ni04028f2.jpg] |
| |||||||||

{kind=link}
{kind=link}