 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
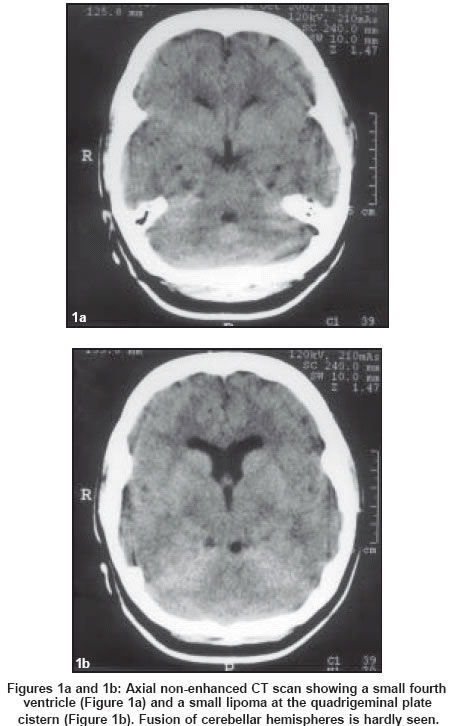
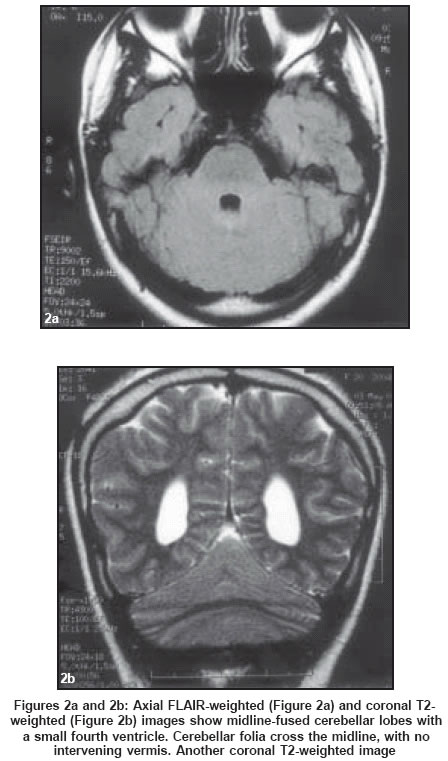
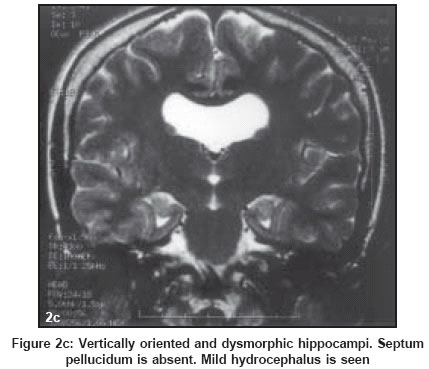
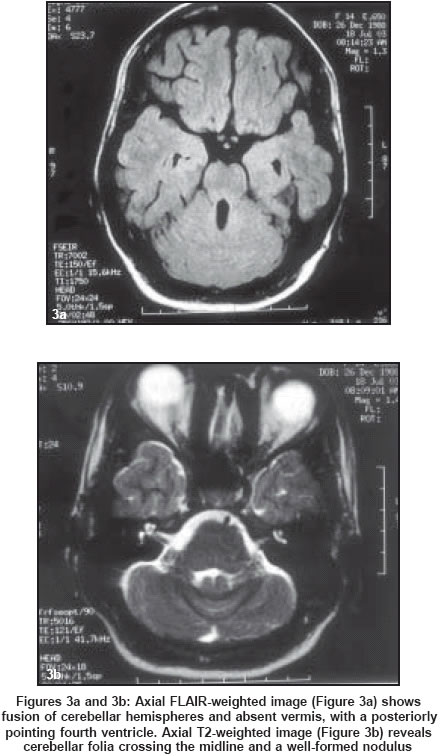
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 118-120 Short Reports Rhombencephalosynapsis: CT and MRI findings Mendonça JL, Natal MR, Viana SL, Coimbra PP, Viana MA, Matsumine M Clinica Radiologica Vila Rica; Unimed Brasilia Code Number: ni04032 Abstract An unusual disorder of cerebellar development, rhombencephalosynapsis is a unique entity which presents with cerebellar fusion and absence of cerebellar vermis on imaging studies, often associated with supratentorial findings. No specific clinical syndrome has been described in these patients so far, and most cases are found in infancy and childhood. MRI and its multiplanar capabilities and high spatial and contrast resolution increased its recognition. Two cases are reported, with emphasis on imaging findings. Introduction Rhombencephalosynapsis (RS) is an uncommon malformation of the posterior fossa characterized by hypoplasia or aplasia of the vermis and fused cerebellar hemispheres; fusion or apposition of the dentate nuclei and cerebellar peduncles are also observed. The clinical course is variable and depends on the severity of the posterior fossa findings and supratentorial-associated anomalies. It has been increasingly reported since the advent of MRI, although there are no more than 40 cases described. In this paper, we report CT and MRI findings of one adult patient and MRI findings of one teenager with RS, reviewing the literature about this rare condition. Case Reports Case 1 A previous CT scan was interpreted as normal. A cranial MRI was performed. CT scan, retrospectively analyzed with the benefit of MRI images showed a small fourth ventricle, associated with the absence of the septum pellucidum and a small hypodense lesion at the quadrigeminal plate cistern, slightly left to the midline. Fusion of the cerebellar lobes was hard to see on CT scan images [Figure:1a] and [Figure:1b]. On MRI, besides CT scan findings, cerebellar lobes were fused, with a hypoplastic vermis and transversely oriented folia and fissures; nodulus appeared to be formed [Figure:2a] and [Figure:2b]. The quadrigeminal plate cistern lesion showed high signal on all sequences, compatible with a lipoma. Mild supratentorial hydrocephalus was present. Dentate nuclei appeared apposed. There were dysmorphic, vertically-oriented hippocampi and a thin corpus callosum [Figure:2c]. Case 2 MRI images showed fused cerebellar hemispheres, with horizontally oriented cerebellar folia crossing the midline secondary to vermian agenesis. The fourth ventricle was oval and posteriorly pointing. Nodulus was formed [Figure:3a] and [Figure:3b]. A thickened gyrus was identified at the posterior portion of the left temporal lobe and was interpreted as focal cortical dysplasia. No other supratentorial anomalies were found. Discussion Rhombencephalosynapsis (RS) is a rare cerebellar malformation, first described by Obersteiner, in 1914 (a postmortem description of a 28-year-old man),[1] and it is characterized by the absence or hypogenesis of the vermis and the midline fusion of the cerebellar hemispheres into a single mass. Unlike other vermian maldevelopment syndromes (such as Dandy-Walker complex, Joubert syndrome or tectocerebellar dysraphia), there is no disconnection of cerebellar hemispheres, rather they continue seamlessly through the midline. Some authors believe that this anomaly is not secondary to a primary maldevelopment of the vermis, but rather, results from a primary failure of vermian differentiation. Thus, there would be undivided hemispheres instead of fused ones,[2] possibly due to defective gene expression in early patterning centers of the brain.[3] The pathogenesis is related to a disturbed development of the cerebellum between 28 and 41 days of gestation.[4] However, to this date, true causative factors remain controversial. There is no specific syndrome associated with this condition, so clinical findings may vary, and may be related to posterior fossa pathology, associated supratentorial anomalies.[5],[6],[7],[8] Patients with supratentorial anomalies and rudimentary cerebellum seem to be the most symptomatic ones.[5],[9] Manifestations include hypotonia, motor and cerebellar dysfunction, strabismus and developmental delays.[10] The largest series described so far (nine patients) showed a wide range of findings, varying from mild truncal ataxia and normal intelligence to cerebral palsy.[7] Many patients die in infancy or early childhood, and most reports are of pediatric patients, although there are scattered cases of adult subjects in the literature.[6],[10] No correlation between neuroimaging findings and clinical manifestations could be made so far. The most distinctive feature is agenesis or poor differentiation of the vermis, the rostral portion being the most severely affected, while the caudal vermis is better formed, usually with a well-developed flocculonodulus. Cerebellar hemispheres appear midline fused, with no intervening cyst; folia and fissures are transversely oriented (single-lobed cerebellum). Diagnosis is best made by axial images demonstrating the fused hemispheres, while coronal images show horizontal folial orientation.[7] Superior and middle cerebellar peduncles may be fused, as well as the dentate nuclei and the inferior colliculi, leading to a characteristic diamond-shaped fourth ventricle (narrowed and posteriorly pointing);[2],[10] however, this finding is not so constant.[7] In addition, fusion of the cerebellar peduncles may be difficult to assess in the absence of a high-resolution volumetric sequence.[3] Olivary nuclei may be hypoplastic or absent. Hydrocephalus is the most frequently found supratentorial anomaly and may be associated with aqueductal stenosis. Other supratentorial findings include fused thalami, fornices and cerebral peduncles, absence of the septum pellucidum, dysgenesis of the limbic system, cortical malformations and multiple suture synostoses. Associations with septo-optic dysplasia and holoprosencephaly have already been suggested.[4],[11] Until MRI was available (first descriptions of RS in vivo in 1991),[4],[12] only a few cases were reported (formerly diagnosed only at necropsy); MRI made more in vivo diagnoses of this entity in the last 12 years than all post-mortem examinations from 1914 to 1991. To our knowledge, no case was diagnosed based upon CT findings solely. MRI is clearly superior in evaluating these patients, although CT may theoretically suggest the diagnosis by depicting the characteristic configuration of the fourth ventricle, which lacks the normal cerebellar vallecula, especially if associated with supratentorial anomalies.[5] On MRI, cerebellar folia and fissures transversely oriented across the midline without the intervening vermis, associated with a diamond-shaped fourth ventricle are characteristic, and should prompt search for other supratentorial and infratentorial findings. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04032f3.jpg] [ni04032f2c.jpg] [ni04032f2a-b.jpg] [ni04032f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}