 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
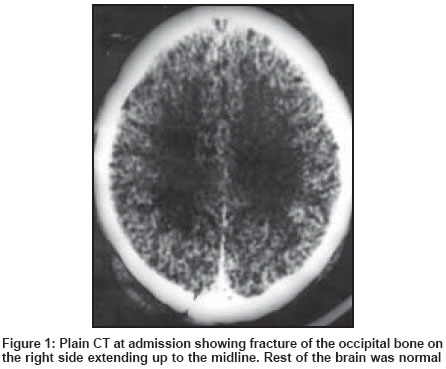
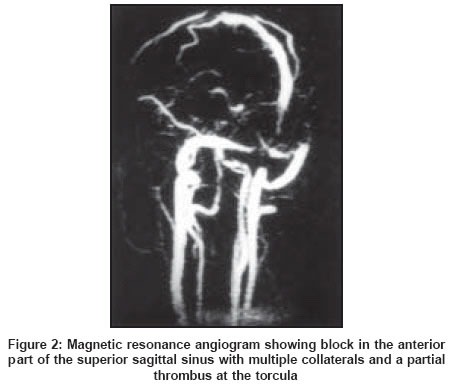
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 123-124 Short Reports Superior sagittal sinus and torcula thrombosis in minor head injury Kumar GSS, Chacko AG, Chacko M Department of Neurological Sciences, Christian Medical College and Hospital, Vellore - 632004 Code Number: ni04035 Abstract A 27-year-old man suffered a relatively minor trauma. He developed signs of raised intracranial pressure three days after injury. Investigations revealed superior sagittal sinus and torcular thrombosis.Introduction Post-traumatic superior sagittal sinus and torcula thrombosis is rare. Various mechanisms in its pathogenesis have been postulated but mortality and morbidity remain high. We report such a case and discuss the treatment protocol. Case Report A 27-year-old man presented a few hours after a head injury and brief loss of consciousness. When admitted he was irritable but had no focal neurological deficits. There was a scalp laceration in the midline occipital region with an underlying linear fracture. The laceration was sutured and he was admitted for observation as the fracture line extended across the sagittal sinus. A plain computed tomogram (CT) of the brain showed a crack fracture of the occipital bone on the right side, which extended to the midline. Rest of the brain was normal [Figure - 1]. Seventy-two hours after the trauma he developed headache and vomiting and developed bilateral sixth cranial nerve pareses. Fundoscopy revealed papilledema. A magnetic resonance angiogram (MRA) showed a block in the anterior third of the superior sagittal sinus and a thrombus partly occluding the confluence of sinuses [Figure - 2]. The patient was placed on anticonvulsants and anti-edema drugs and heparin with which his symptoms improved over five days. Heparin was then changed to oral anticoagulants and he was discharged when he was asymptomatic. Discussion Thrombosis of the superior sagittal sinus (SSST) and torcula is rare and is usually attributed to scalp or skull infections, oral contraception, dehydration, pregnancy, blood dyscrasias and metabolic derangements.[1],[2] Although post-traumatic SSST has been reported, it still remains an unusual complication of traumatic brain injury. The high mortality rate (40%-80%)[3] stresses the need for early diagnosis and treatment. The diagnosis is based on a high index of clinical suspicion, confirmed by imaging. General symptoms and signs are headache and seizures due to cerebral venous infarcts.[4] Buonanno et al[3] reported 11 cases of SSST diagnosed with CT and later confirmed by angiography or autopsy. A reliable finding on CT is the "empty triangle" sign seen on contrast films in the cuts slicing perpendicularly across the posterior aspect of the sinus. The "empty triangle" is due to the presence of an isodense clot within the sinus enclosed by an area of engorged vessels. Less specific findings include small ventricles, gyral enhancement in a distribution of venous infarct and multiple focal bilateral parasagittal hemorrhages. The pathogenesis of SSST is not well established. Carrie and Jaffe[5] state that abnormalities in the clotting mechanism, disturbances in blood flow or damage to the capillary endothelium may predispose and lead to thrombosis. Alteration in coagulation after head injury has been documented supporting this hypothesis.[6] Treatment includes maintaining good hydration, and the administration of anti-edema agents like dexamethasone and mannitol. Anticonvulsants are necessary to prevent seizures. There are reports of the successful management of SSST with heparin and urokinase, including the restoration of the patency of the sagittal sinus with continuous urokinase infusion directly into the sinuses via a transfemoral transvenous microcatheter.[7],[8] References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04035f1.jpg] [ni04035f2.jpg] |
| |||||||||

{kind=link}
{kind=link}