 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
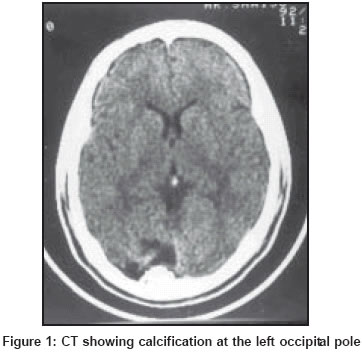
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 130 Letter To Editor Calcified occipital glioblastoma Bhatoe HS, Kumar H Departments of Neurosurgery, Army Hospital (R & R), Delhi Cantt - 110010 Code Number: ni04043 Sir, A rare case of a glioblastoma having areas of calcification is reported. The relevant literature is briefly reviewed. An 18-year-old-boy was admitted with a one-month history of bifrontal headache, intermittent vomiting and diplopia. He had history of seizures since the age of four years. The seizures were not preceded by any aura and the ictus consisted of a blank expression lasting for a few seconds. His scholastic performance had been average. Clinical examination revealed bilateral abducens paresis and mild papilledema. There was right-sided homonymous hemianopia. There was no cognitive deficit, disconnection syndrome or motor weakness. Skull radiograph and CT [Figure - 1] done three years earlier had revealed calcification at the left occipital pole, without any mass effect. CT done at the time of present admission showed a large, mixed, attenuating and partly enhancing lesion at the left occipital pole having areas of calcification. Left occipital craniotomy and a radical resection of the tumor-bearing occipital pole was carried out. The tumor was firm, solid and gritty and was not very vascular. The postoperative period was uneventful. Histopathology revealed a highly cellular tumor made up of anaplastic and pleomorphic cells with several mitotic figures and bizarre giant cells. Astrocytic proliferation was seen in the peripheral areas. There were areas of necrosis with palisading of nuclei and angioendothelial proliferation. Many areas of calcification were seen. The tumor was positive for glian fibrillary acid protein (GFAP). A diagnosis of glioblastoma multiforme with calcification was made. The lesion was then subjected to radiotherapy and chemotherapy. The patient was free from recurrence for three years after surgery, after which he was lost to follow-up. Calcification may be seen in gliomas, especially in oligodendrogliomas and in mixed gliomas that have a benign histological appearance. It is unusual in high grade astrocytomas and glioblastomas; it is likely that some part of the previously low grade tumor may dedifferentiate into glioblastoma.[1],[2],[3],[4] Histological markers suggesting a better prognosis in gliobalstomas include presence of giant cells and differentiation. The presence of calcium deposits has rarely been recorded.[3] References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04043f1.jpg] |
| |||||||||

{kind=link}