 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
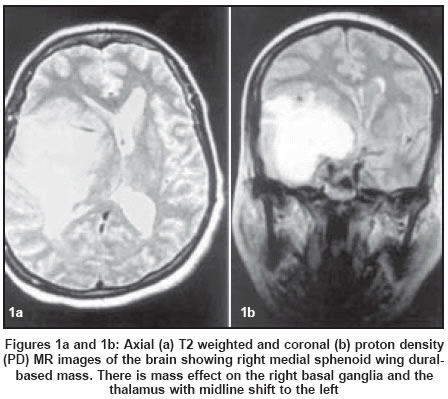
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 133 Letter To Editor Sphenoid wing meningioma presenting as hemi-parkinsonism: Case report Shah KC, Rajshekhar V Department of Neurological Sciences, Christian Medical College Hospital, Vellore Code Number: ni04047 Sir, Parkinson′s disease (PD) has infrequently been described in association with intracranial tumors.[1],[2],[3],[4] We describe a patient who had a sphenoid wing meningioma and presented with hemi-parkinsonism. Parkinsonism was completely relieved after tumor resection. A 54-year-old woman presented with a 2-month history of tremor, particularly at rest, in the left upper limb and 2 episodes of generalized seizures. Examination revealed a masked facies, rest tremor in the left hand with a postural tremor of small amplitude, cog- wheel rigidity at the left wrist and elbow and loss of dexterity due to bradykinesia. Fundus showed bilateral papilledema. Gait was normal but slow and left arm swing was diminished. Rest of the neurological examination revealed no abnormality. MRI of the brain showed a large homogenous dural-based mass along the right medial sphenoidal wing with significant perilesional edema and midline shift [Figure - 1]. She underwent right fronto-temporal craniotomy and near-total excision of the tumor. Postoperatively her tremor and rigidity in the left upper limb disappeared completely. Histologically, the tumor was a meningioma. The basal ganglia play a major role in the control of posture and movement. Intrinsic basal ganglionic and thalamic lesions as well as extrinsic compressive lesions have been reported to cause Parkinsonism-like syndrome. Parkinsonism is produced more often by external masses impinging on the basal ganglia than by intrinsic infiltrating lesions. Gliomas, meningiomas, metastatic tumors and even chronic subdural hematoma have been reported to produce symptoms of Parkinsonism.[2],[5] Direct mechanical pressure and/or torsion of the basal ganglia by a tumor might cause dysfunction of these nuclei. The other proposed mechanism is midbrain compression from upward or downward transtentorial herniation.[3] Such herniation may result in the impairment of blood flow to the basal ganglia via the posterior cerebral artery, leading to ischemia of the subthalamic nuclei. In intrinsic tumors, the basal ganglia and thalamus are involved primarily by the tumor, which may lead to internal compression of neurons or pathways. An intracranial mass as a cause of PD might be missed, especially in elderly patients. Associated symptoms of increased intracranial pressure, focal motor or sensory deficits or seizures (as in our patient) can assist in the diagnosis. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04047f1.jpg] |
| |||||||||

{kind=link}