 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
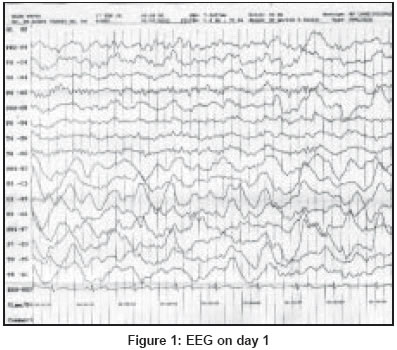
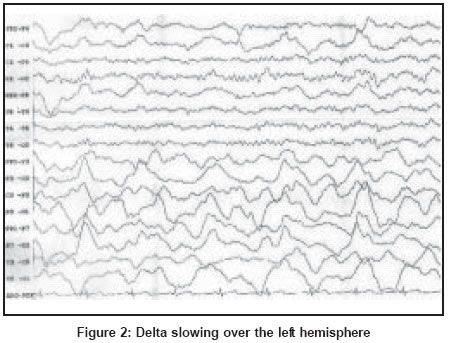
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 134 Neuroimage EEG in hemiplegic migraine Varkey B, Varkey L Indo-American Hospital, Brain and Spine center, Vaikom, Kerala Code Number: ni04048 A 17-year-old boy developed diffuse throbbing headache of 36 hours duration associated with photophobia and phonophobia. Twelve hours later, he developed dysarthria and right-sided weakness. He had a similar episode 5 months ago with resolution of symptoms in 24 hours, following which he was put on prophylactic sodium valproate 300 mg/day. His elder brother had suffered from intermittent diffuse headache associated with numbness of the right-sided limbs. A clinical diagnosis of hemiplegic migraine, probably familial, was made. CT scan and MRI showed no intracranial abnormality. The wake EEG record on Day 1 showed diffuse delta waves at 1-3 Hertz over the left hemisphere, which were prominent posteriorly [Figure - 1] and [Figure - 2]. The background activity was normal over the right hemisphere. Over the next 5 days the EEG changes returned to normal and the patient′s hemiparesis resolved. Hemiplegic migraine is a subtype of migraine and is accompanied by hemiplegia, which may outlast the headache. Hemiplegia is sometimes associated with altered consciousness and aphasia, and rarely with coma. Hemiplegic migraine occurs in two forms-Sporadic hemiplegic migraine and Familial hemiplegic migraine.[1] EEG studies have demonstrated a wide variety of patterns. During the ictus, severe unilateral or focal disturbances-delta-activity, theta-delta-activity, theta-activity or alpha-reduction-are seen. Hemiplegic migraine has shown the most definitely abnormal EEGs.[2],[3] Pseudoperiodic slow sharp waves over the hemisphere contralateral to the hemiplegia have also been recorded. In most cases the changes subside in a few days and the EEG returns to normal. MR imaging during the period of attack shows cerebral edema, dilatation of intracerebral vessels and decreased water diffusion contralateral to the hemiparesis. The MRI changes resolve completely in the post-ictal phase. These results suggest an underlying primary neuronal pathology with secondary vascular effects, as opposed to the traditional, primarily vascular model of migraine etiology.[4] References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04048f2.jpg] [ni04048f1.jpg] |
| |||||||||

{kind=link}
{kind=link}