 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
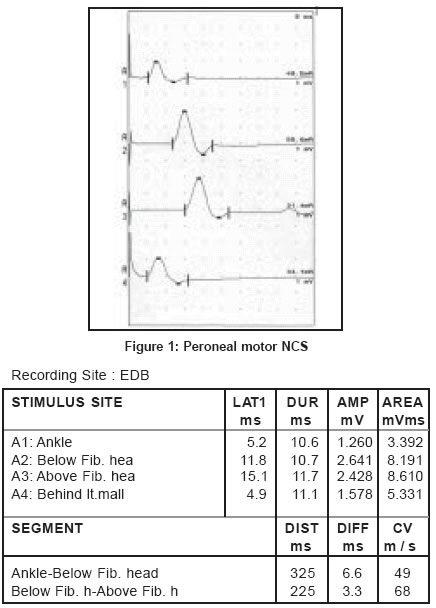
Neurology India, Vol. 52, No. 1, January-March, 2004, pp. 135 Neuroimage Accessory deep peroneal nerve Kuruvilla A Department of Neurology, Sree Chitra Tirunal Institute for Medical Sciences and Technology, Trivandrum - 695 011 Code Number: ni04049 The anomalous innervation of the extensor digitorum brevis (EDB) muscle by the accessory deep peroneal nerve is presented below. This 23-year-old male was referred to the clinical neurophysiology laboratory for evaluation of possible lumbar radiculopathy. The nerve conduction study (NCS) and electromyography revealed abnormalities consistent with an S1 radiculopathy on the right. Incidentally, the routine peroneal nerve conduction study on the left revealed a larger compound muscle action potential (CMAP) on proximal stimulation below and above the fibular head, when compared to the distal stimulation [Figure - 1], trace A2, A3 and A1 respectively). The stimulation behind the lateral malleolus showed a CMAP with amplitude of 1.6 mV [Figure - 1], trace A4), thus confirming the presence of the accessory deep peroneal nerve. The NCS of the right peroneal nerve did not reveal any anomaly. Comments Anatomic variations in the innervation of muscles should be kept in mind during the electrophysiological assessment of neuropathies. Lack of awareness of these anomalies may result in the wrong interpretation of nerve conduction results. The deep peroneal nerve, a major branch of the common peroneal nerve, usually innervates the [EDB]. In 21-28% of subjects, this muscle also receives innervation from the accessory deep peroneal nerve, an anomalous branch of the superficial peroneal nerve.[1] This anomaly should be suspected when proximal stimulation of the common peroneal nerve at the knee elicits higher amplitude CMAP, than stimulation of the deep peroneal nerve at the ankle. Stimulation of the accessory deep peroneal nerve behind the lateral malleolus activates the anomalously innervated lateral portion of the [EDB]. Rarely, this anomalous branch may exclusively supply the [EDB]. In the presence of this anomaly, the lesions of the deep peroneal nerve spare the lateral portion or the whole of the [EDB], thus leading to the possibility of an incorrect conclusion.[2] The inheritance pattern of the accessory deep peroneal nerve shows an autosomal dominant trait.[3] References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04049f1.jpg] |
| |||||||||

{kind=link}