 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
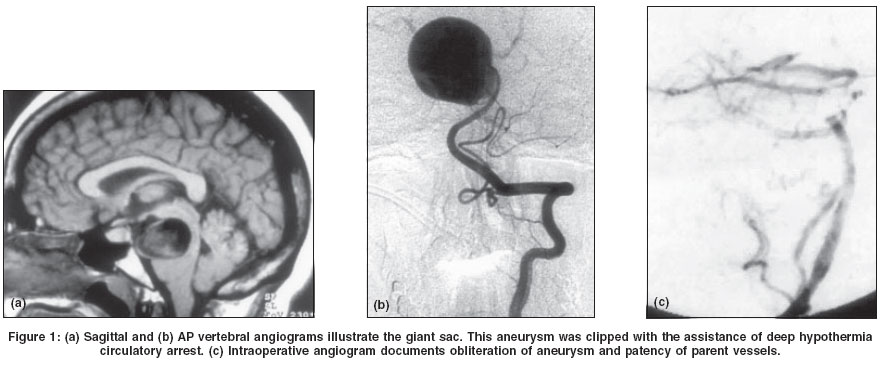
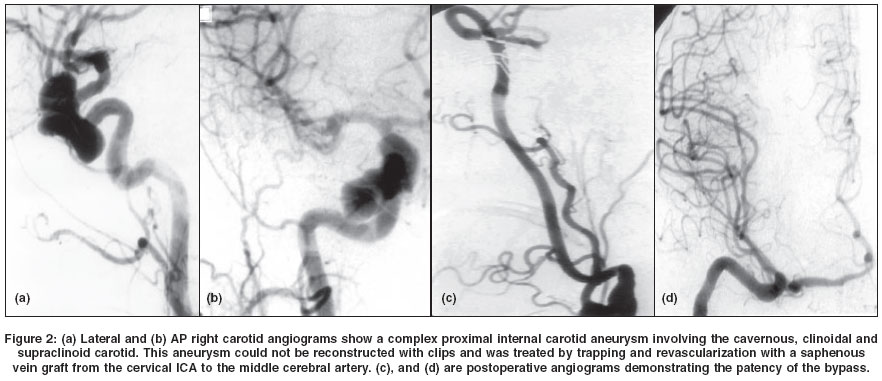
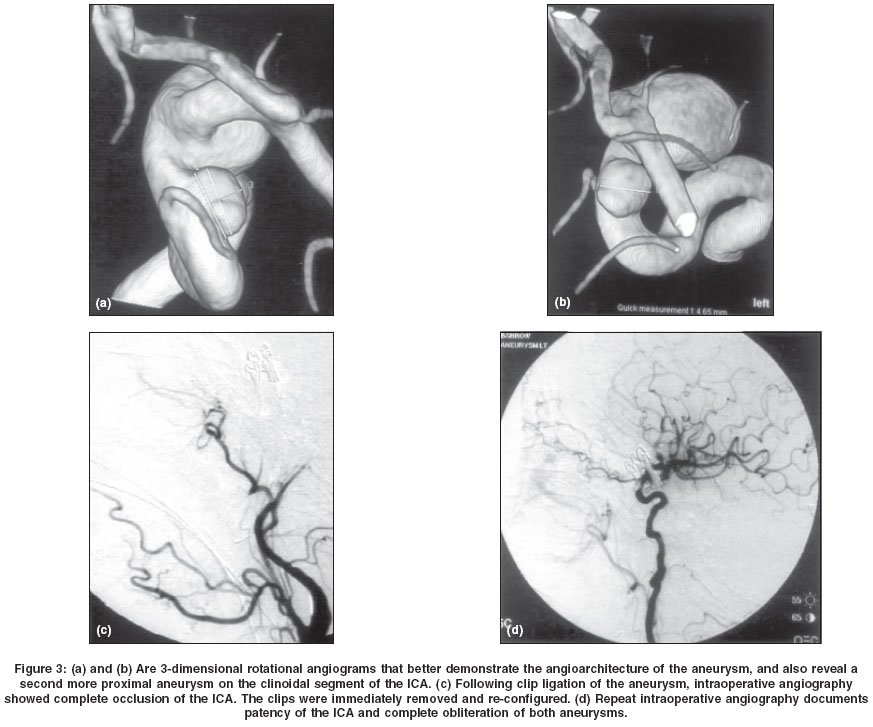
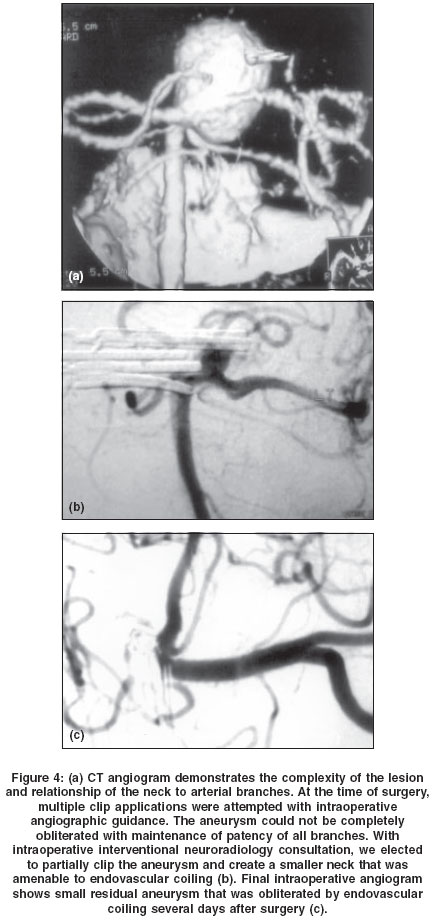
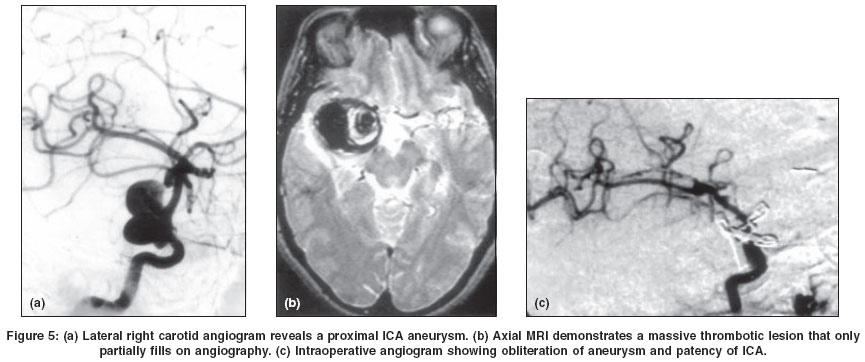
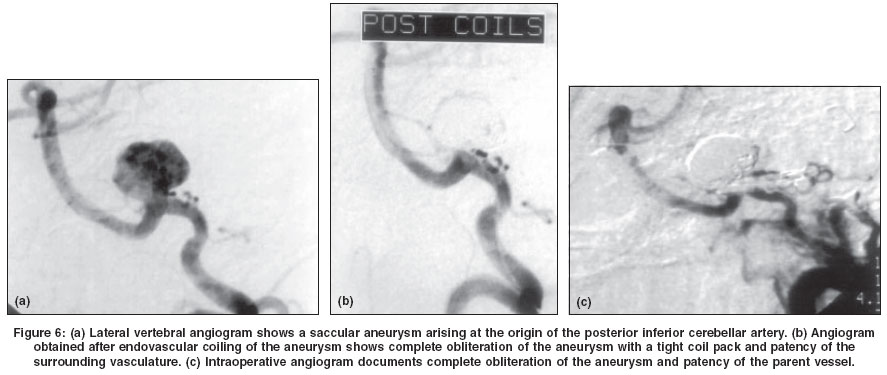
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 156-162 Review Article Surgical management of complex intracranial aneurysms Barrow Daniel L, Cawley CMichael Department of Neurosurgery and Emory MBNA Stroke Center, Emory University School of Medicine, Atlanta, Georgia Code Number: ni04052 ABSTRACT Despite the improvements in increasing popularity of endovascular therapy for intracranial aneurysms, there remain a large number of these lesions that currently are not amenable to endovascular therapy. As endovascular therapy becomes more popular, those aneurysms requiring surgical intervention will become increasingly complex. To manage these challenging lesions, neurosurgeons must use all available innovations and advances, including diagnostic, technical and perioperative adjuncts. In this review article, we discuss limitations of endovascular therapy, the populations of aneurysms that continue to require surgical treatment, the factors that make an aneurysm complex and the multiple adjuncts utilized to successfully treat these challenging lesions. Keywords: Intracranial aneurysms; endovascular therapy; neurovascular susrgery INTRODUCTION The development and refinement of endovascular therapy has provided new strategies for managing intracranial aneurysms. These advances offer a less invasive option for treating aneurysms, and strengthen the therapeutic armamentarium available to the neurovascular team. There remain a significant number of aneurysms for which there is currently no endovascular option that will provide long-term protection against subarachnoid hemorrhage (SAH) or the progressive mass effect of some aneurysms. Therefore, for the foreseeable future, neurovascular surgeons will need to provide surgical treatment for many intracranial aneurysms. Currently, endovascular therapy is ideally suited for those aneurysms that are most readily treated by surgery. As endovascular therapy is used for an increasing number of aneurysms, surgery will be required for the treatment of an increasingly more complex population of aneurysms. Neurosurgeons must utilize all the innovations and advances of our specialty to successfully manage this challenging group of patients. Limitations of Endovascular Therapy The primary benefit of endovascular therapy is the fact that it avoids a surgical procedure. It is less invasive, well tolerated and requires significantly less recovery time than surgery. This is particularly important for patients with unruptured aneurysms, whose hospitalization and recovery can be significantly shorter after endovascular treatment. For a patient who has experienced a SAH, the length of hospitalization and recovery is dictated more by the SAH than the mode of treatment. Despite the benefit of minimal invasiveness, endovascular therapy has a number of detractors, including risks, inferior durability compared to surgical clip ligation, the need for long term follow up, and lack of universal applicability to all aneurysms. There are a large number of intracranial aneurysms for which current endovascular techniques are unsuitable. The remaining challenges for endovascular therapy include certain locations such as the middle cerebral artery (MCA) or distal location on a parent artery, wide necked, fusiform or complex configuration, giant size, intraluminal thrombus and failure to consistently eliminate mass effects. Endovascular therapy is usually contraindicated in patients with a large or life-threatening hematoma. Although continued advances in endovascular technology will address many of these challenges, neurosurgeons will be required to manage an increasingly complex population of lesions that are recalcitrant to current endovascular technologies.[1] Furthermore, the ability of endovascular techniques to provide permanent obliteration of aneurysms remains to be demonstrated. The International Subarachnoid Aneurysm Trial (ISAT) demonstrated the ability of endovascular therapy to provide short-term treatment of aneurysms with less morbidity than surgical repair.[2] Despite a number of legitimate criticisms of the study, we believe the publication of this trial will lead to an increased use endovascular therapy to treat aneurysms. Surgical Adjuncts Diagnostic Technical The principles of skull base surgery are to utilize a refined knowledge of anatomy to create surgical approaches that sacrifice bone of the skull base to minimize retraction of neural tissue and to create corridors that bring the surgeon closer to the target pathology. Although initially developed for neoplastic pathology involving the skull base, these techniques have been adapted for vascular neurosurgery, particularly in the treatment of intracranial aneurysms. Examples of standard utilization of skull base surgical techniques include anterior clinoidectomy for proximal ICA aneurysms, orbitozygomatic extension of the pterional approach for basilar bifurcation aneurysms associated with a high basilar bifurcation, medial petrosectomy for basilar bifurcation aneurysms associated with a low basilar bifurcation and transcondylar approach for aneurysms arising on the vertebral artery up to its confluence. A thorough knowledge of skull base surgical techniques is essential for the modern management of many intracranial aneurysms. A number of intracranial aneurysms are unable to be safely clipped in their fully inflated state. Furthermore, the final stages of dissection of many other aneurysms can be made safer by temporarily interrupting blood flow to the sac. By utilizing current knowledge of brain protection, one can prolong the period of time the brain can tolerate temporary occlusion of the afferent and efferent arteries of an aneurysm. Such adjuncts include moderate hypothermia, barbiturates or etomidate to decrease brain metabolism, mannitol to improve rheology in the microcirculation and induced hypertension to augment collateral flow. In extreme cases, deep hypothermic circulatory arrest can markedly prolong the duration of cessation of blood flow yet protect the brain from ischemia [Figure - 1]. Knowledge of these adjuncts and judicious use of temporary local or global interruption of cerebral blood flow can assist in increasing the number of intracranial aneurysms amenable to surgical cure.[4] Currently, a wide variety of aneurysm clips are available to reconstruct even the most refractory and complex sacs. Modern clips have high closing pressures to ensure long-term efficacy and durability. All imaginable angles, lengths and designs, including fenestrated clips, provide an endless variety of reconstruction options for eliminating complex aneurysms from the intracranial circulation. For those extraordinarily complex aneurysms that are simply not amenable to clip ligation with preservation of the parent artery and its branches, the modern neurovascular surgeon must be comfortable with various extracranial-intracranial (EC-IC) bypass techniques. The option of parent vessel occlusion or aneurysm trapping with surgical revascularization will allow the surgeon the ability to address a number of highly complex aneurysms in a definitive manner [Figure - 2]. The goals of aneurysm surgery are to eliminate the aneurysm from the intracranial circulation and maintain patency of the parent vessel and its branches. Achievement of these goals can be confirmed by direct observation through the operating microscope or the use of postoperative angiography. The former method may be inaccurate and misleading, while the latter may provide information at a time when it is too late to correct the problem. The combination of intraoperative angiography and microvascular Doppler provide the opportunity to confirm that the goals of the neurovascular procedure have been achieved while the patient is still under anesthesia and any shortcomings can be rapidly addressed [Figure - 3]. Perioperative Endovascular therapy has also played an important role in the surgical management of patients with intracranial aneurysms. Endovascular balloon angioplasty is an important adjunct in the management of medically refractory cerebral vasospasm. We and others have found endovascular therapy to be a useful adjunct in occasional patients whose aneurysms proved to be unsuitable for either surgical clipping or endovascular therapy. Occasionally, these refractory lesions can be converted by surgical means into a lesion that is now treatable by endovascular techniques [Figure - 4]. A final "adjunct" that should be discussed is experience. There is now ample data to demonstrate that volume-outcome relationships exist for many surgical procedures including aneurysm surgery.[7],[8],[9],[10] It has been clearly demonstrated that those institutions with higher volumes of aneurysm surgery have better outcomes and highest likelihood of definitive treatment. Therefore, we believe regionalization of aneurysm surgery is an essential component of an effort to decrease morbidity and improve outcome. Definition of Complex Aneurysms There are numerous factors that make a given intracranial aneurysm "complex." These factors include location, configuration, size, and presence of intraluminal thrombus and/or calcification. Additionally, intraoperative misadventures may convert a "straightforward" aneurysm into a "complex" aneurysm. Finally, failed prior surgical attempts or failed endovascular therapy may make an aneurysm "complex."Location Adjuncts that are useful in managing aneurysms in difficult locations include skull base techniques to improve exposure and intraoperative angiography plus microvascular Doppler to document obliteration of the aneurysm and maintenance of patency of the parent vessels and their branches. Configuration Size For selected giant aneurysms, particularly those in the posterior circulation, prolonged interruption of blood flow into the aneurysm will be required. Occasionally, this requires use of deep hypothermic circulatory arrest. Availability of a variety of modern, high-closing pressure aneurysm clips is essential for the reconstruction of large or giant aneurysms. Familiarity with creative clip constructions, including use of fenestrated clips and tandem clipping techniques is essential. Confirmation of achievement of goals by intraoperative angiography is of particular importance when dealing with large aneurysms. At the other extreme, very small aneurysms may be quite difficult to obliterate with a clip. If an aneurysm is too small to accept a clip, the surgeon must be creative in dealing with the lesion. Careful bipolar coagulation under constant irrigation will often thicken the wall of the aneurysm. Some of these small sacs can be treated by an encircling Sundt clip-graft, or by creating a "sling" of muslin around the aneurysm and parent artery and securing it with an aneurysm clip.[11] Intraluminal Thrombus and/or Calcification Thrombotic aneurysms often have thick necks that may require aneurysm clips with high closing pressure, such as Sundt-Kees clips. Tandem clipping techniques with fenestrated clips are another method of increasing the closing pressure of the clip application. Calcification of the dome of an aneurysm can be managed in much the same way as intraluminal thrombosis. Calcification of the aneurysm neck, however, is more problematic. Dense calcification of the neck usually will prevent the aneurysm clips from closing completely. Occasionally, the deposits of calcium can be removed during temporary occlusion under brain protection and after opening the aneurysm. This maneuver, however, carries a significant risk of damaging the parent artery and occasionally the vessel literally falls apart. More often, the calcified neck can be carefully crushed with a small pair of rubber-shod hemostats. This will prepare the neck to accept the clip and close completely. There is certainly some risk to this maneuver and intraoperative angiography is strongly recommended to document patency of the parent vessel. The surgeon dealing with thrombotic or calcified aneurysms should be prepared to perform an EC-IC bypass if patency of the parent vessel and its branches cannot be maintained and there is inadequate collateral circulation. Intraoperative Misadventures Intraoperative rupture of an aneurysm is relatively straightforward to deal with if it occurs after the aneurysm is exposed. The bleeding site is usually readily controlled with a small piece of cotton placed over the site with suction. The application of temporary clips can then reduce or eliminate the bleeding during definitive clipping. Intraoperative rupture in the early stages of exposure can be catastrophic. Keeping calm and following the jet of blood to the source with a large-bore suction will often control the bleeding and allow the surgeon to apply temporary clips. The successful management of an intraoperative rupture or other misadventure requires the use of all operative adjuncts and frequently the application of a creative solution. Failed Prior Therapy From January 1995 to 2001, we treated 72 aneurysms in 67 patients at Emory University Hospital in which surgical therapy has been necessary following incomplete surgical and/or endovascular intervention. Thirty-three of these aneurysms were small (<10mm), 25 were large (10-25mm), and 14 were giant (>25mm). Thirty-five aneurysms in 32 patients were previously treated by surgery and experienced recurrences. Thirty of these aneurysms were in the anterior circulation and 5 in the posterior circulation. All aneurysms were obliterated as documented with intraoperative and/or postoperative angiography. Eighty one percent of these patients experienced a favorable outcome as determined by the Glasgow outcome scale (GOS). There were 2 mortalities and 7 patients experienced some transient surgical morbidity. During the same time period, 37 aneurysms were treated in 35 patients who had undergone failed endovascular therapy. Twenty-four aneurysms were located in the anterior circulation and 13 in the posterior circulation. Thirty of these aneurysms were clipped. Four lesions required trapping, 3 with EC-IC bypass. Two parent vessel occlusions were required and one aneurysm was reinforced with muslin. Two of these patients required deep hypothermic cardiac standstill to treat their aneurysms. In the group previously treated with endovascular therapy, 27 patients resumed normal life. Three patients had moderate disability but were independent. Two patients were severely disabled and there were 3 mortalities. CONCLUSION The microsurgical treatment of intracranial aneurysms will be necessary for the foreseeable future. One can anticipate that with further advances in endovascular therapy, an increasing number of aneurysms will be amenable to endovascular therapy. The durability of these treatments, however, remains unproven. As endovascular techniques gain popularity, aneurysms presenting for surgical management will become increasingly complex and the ability of cerebrovascular neurosurgeons will continue to be tested. REFERENCES
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04052f3.jpg] [ni04052f5.jpg] [ni04052f2.jpg] [ni04052f4.jpg] [ni04052f6.jpg] [ni04052f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}