
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 178-184
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 178-184
Original Article
Vertebral artery in relationship to C1-C2 vertebrae: An anatomical study
Cacciola Francesco , Phalke Umesh , Goel Atul
Department of Neurosurgery, Seth G. S. Medical College and King Edward Memorial Hospital, Parel, Mumbai
Correspondence Address:Department of Neurosurgery, King Edward Memorial Hospital, Parel, Mumbai
atulgoel62@hotmail.com
Code Number: ni04055
Abstract
BACKGROUND: Ten randomly selected adult cadaveric specimens were dissected to analyse the anatomy of the vertebral artery during its course from the C3 transverse process to its entry into the spinal dural canal at the level of C1. In addition, 10 dry cadaveric C1-C2 bones were studied. The course of the artery and the parameters relevant during surgery in the region are evaluated. METHODS: Ten adult cadaveric specimens and 10 adult dry cadaveric C1 and C2 bones were studied. In five cadaveric specimens, the arteries and veins were injected with coloured silicon. The artery during its course from the transverse process of C3 to the transverse process of C2 was labelled as V1 segment, the artery during its course from the C2 transverse process to the C1 transverse process was labelled as V2 segment and the segment of the artery after its exit from the transverse foramen of C1 to the point of its dural entry was labelled as V3 segment. The relationship of the artery to the C1-2 joint and facets, distance of the location of the artery from the midline, from the C2 ganglion and from the other surgery related landmarks were evaluated. The extent of occupancy of the artery into the vertebral artery groove on the inferior surface of the superior facet of the C2 vertebra, and over the posterior arch of the atlas was studied. RESULTS: The V1 segment of the vertebral artery takes a varying degree of loop inside the vertebral artery foramen on the inferior aspect of the superior facet of the C2 vertebra. The loop extends towards the midline and was at an average distance of 14.6 mm from the midline of the vertebral body. The V2 segment of the artery takes an initial lateral loop after its exit from the transverse process of the C2 vertebra. The average distance of the artery from the lateral end of the C2 ganglion was 7.2 mm and from the dural tube was 15.3 mm. The vertebral artery groove in the superior facet of C2 and the groove over the posterior arch of the atlas were completely occupied by the vertebral artery only in six sides and in none respectively, suggesting the possibility of the dynamic nature of the relationship of the artery to the bone. CONCLUSIONS: The vertebral artery adopts a serpentine course in relationship to the C2 vertebra, making it susceptible to injury during the surgical procedures in the region. The multiple loops of the artery and a buffer space within the vertebral artery groove on the inferior surface of the superior facet of the C2 vertebra and over the posterior arch of atlas provide the artery an extra length and space, probably essential to avoid any stretch during neck movements.
Keywords: Vertebral artery, C2-ganglion, atlas, axis, craniovertebral junction
Introduction The anatomy of the vertebral artery in the region of the craniovertebral junction is significantly different from the relatively straightforward course in the transverse foramina of C6 to C3 vertebrae. A three-dimensional understanding of the anatomy is crucially important for any kind of surgery in the craniovertebral region. Various authors have reported incidence of vertebral artery injury during transoral surgery, lateral mass and transarticular screw implantation for atlantoaxial fixation and during lateral approaches to the foramen magnum region.[1],[2] The present study is designed to address a number of clinically relevant parameters pertaining to the vertebral artery in relationship to the C1 and C2 vertebrae. The nomenclature of various bony components of the C2 vertebra has been used differently by various authors.[3],[4],[5],[6] We followed the nomenclature clarified by Benzel.[3] Material and methods
Ten adult cadaveric specimens were examined using magnification (x 6-40). In five specimens coloured silicone was injected in the arteries and veins. The microsurgical anatomy of the vertebral artery was evaluated along its course from the C3 transverse process to its entrance into the spinal canal at the C0-C1 level with particular attention to its relationship with the bony structures. For this purpose the bony groove of the artery on the inferior surface of the superior facet of C2 was unroofed. In addition, 10 dry C1 and C2 bones were studied. All measurements were made using a digital calliper and a goniometer. The findings were then corroborated with measurements on the images loaded on the computer [Figure - 1], [Figure - 2], [Figure - 3], [Figure - 4], [Figure - 5]. Results Anatomical considerations
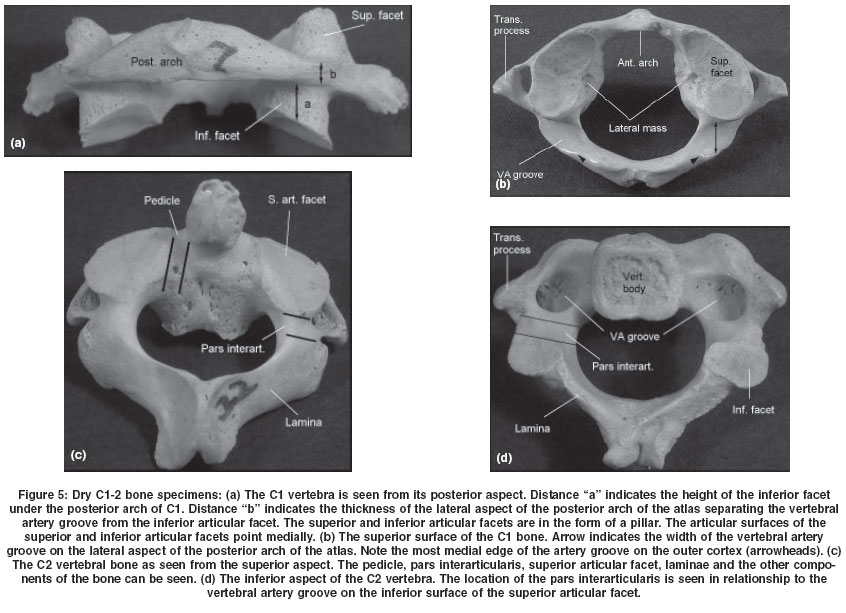
Osseous anatomy [Figure - 5]: The superior facet of the atlas was of oval shape with a groove on either side (76%) and was kidney shaped in 24 facets, wherein the groove was only on one side of the facet. Anteroposterior dimension (mean 19.73 mm) was more than transverse dimension (mean 11.12 mm) in all superior facets of the atlas. None of the superior facets of atlas was found to be exactly symmetrical to that on the contralateral side. Both superior and inferior facets of the atlas always faced medially towards the spinal canal. The inferior facet of the atlas was almost circular in most of the vertebrae without any significant difference in the mean anteroposterior (15.76 mm) and transverse (15.22 mm) dimensions. The thickness of the inferior facet under the posterior arch of the atlas was 1.7 mm to 5.2 mm (average 3.5 mm). The thickness of the posterior arch of the atlas separating the vertebral artery groove from the inferior facet was 2.2 mm to 4.8 mm (average 3.8 mm). The vertebral artery foramen was in the transverse process lateral to the lateral mass of the C1 vertebra [Figure - 5]. The groove for the vertebral artery on the superior surface of the posterior arch of the atlas was converted into a complete bony foramen in one of the twenty sides examined. The distance from the midline to the medial-most edge of the vertebral artery groove on the outer cortex of the posterior arch was 14.3 mm to 19.7 mm (average 18.2 mm).
The axis vertebral body has a thick and conical superior projection of the dens. The dens is flanked by two large, superior facets, extending laterally on to the adjoining pars-interarticularis and articulating with the inferior atlantal facets. Unlike superior facets of all other vertebrae, they do not form a pillar with the inferior facets, being considerably anterior to these. The shape of the articular surface of the superior facet of the axis varied. In 54% facets it was oval with anteroposterior dimension more than transverse, in 27% facets it was oval with transverse dimension more than anteroposterior dimension and in 19% facets it was circular. It was convex in the sagittal plane and was directed laterally to articulate with inferior facet of C1. The average depth of the vertebral artery groove on the inferior surface of the superior facet was 4.36 mm (range 2-8.2 mm). The vertebral artery groove extended in the superior facet up to its medial third in 10 cases, middle third in 18 cases and up to its lateral third in 12 cases. In none of the specimens did the vertebral artery groove extend in to the body of axis vertebra or into the pars interarticularis. The vertebral artery groove was located 2.2 mm to 3.4 mm (average 2.8 mm) anterior to the anterior limit of pars interarticularis. The transverse thickness or the width of pars interarticularis ranged from 5.8 mm to 11.4 mm (average 7.9 mm). The total length of the pars interarticularis ranged from 12.3 mm to 19.4 mm (average 15.3 mm). The angle of pars interarticularis projection towards the superior facet was measured as the angle of pars interarticularis from the vertical plane. It ranged from 38.2 degrees to 50.1 degrees (average 42.3 degrees).
The intertransverse process height between C1 and C2 ranged from 14.7 mm to 18.4 mm (average 17.5 mm). The intertransverse process height between the C2 and C3 transverse processes ranged from 6.4 mm to 14.6 mm (average 11.3 mm). Vascular anatomy:
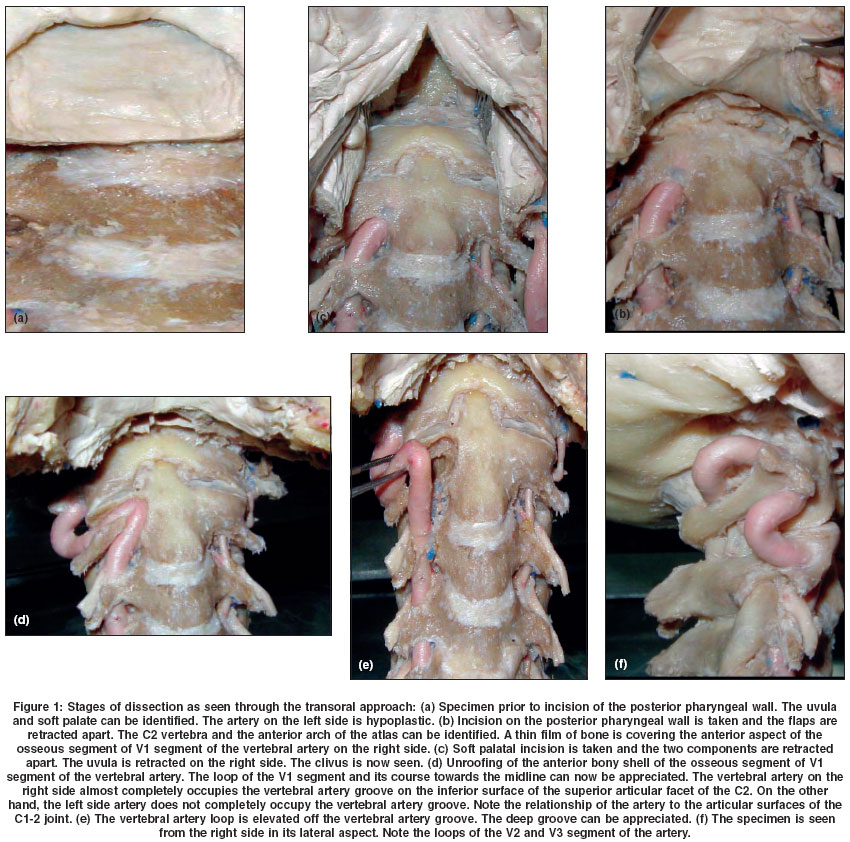
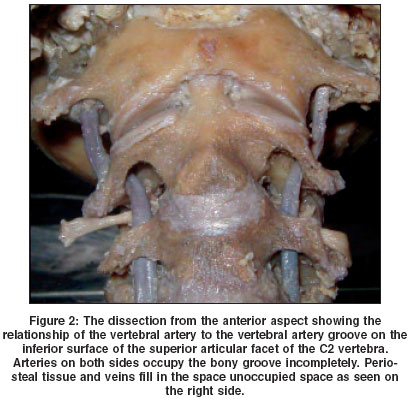
[Figure - 1], [Figure:2], [Figure - 3] The vertebral artery during its entire course was covered with a large plexus of veins. The venous plexuses were the largest in the region lateral to the C1-2 joint. The diameter of the vertebral artery ranged from 2.3 mm to 7.4 mm (average 4.2 mm). The dimensions of the left side artery ranged from 2.3 mm to 4.5 mm whilst that on the right side artery ranged from 4.1 mm to 7.4 mm. In one specimen, there was a marked difference in the size of the artery on the left and right side, the artery on the left side being significantly hypoplastic [Figure - 2]. To assist in the description, the vertebral artery from its course from the C3 transverse foramina to the C2 transverse foramina was labelled as V1, the artery during its course from C2 transverse foramina to C1 transverse foramina was labelled as V2 and the artery in its course from the transverse foramen of C1 to the point of its dural entry was labelled as V3 segment. V1- segment:
After its exit from the transverse foramen of the C3 vertebra, the V1-segment of the artery courses posterosuperiorly forms a loop within the vertebral artery groove on the inferior surface of the superior articular facet, and then exits from the transverse foramina of the C2 vertebra. The total length of the segment ranged from 17.2 mm to 46.1 mm (average 23.4 mm). The distal part of the artery was intraosseous and could not be seen until its bony unroofing. The length of the artery prior to its entry into the osseous compartment was 6.4mm to 14.6 mm (average 11.3 mm). The length of the osseous segment of the artery was 8.5 mm to 36.2 mm (average 14.8 mm). The artery courses medially and takes a reverse loop inside the vertebral artery bony foramina on the inferior surface of the superior facet of the C2 vertebra. The angle of the loop varied and ranged from 2 to 110 degrees (average 86 degrees). More than 75% of transverse extent of the superior facet was occupied by the artery in 2 cases, 50-75% of the facet was occupied by the artery in 5 cases, 25-50% facet was occupied by the artery in 8 cases and less than 25% facet was occupied by the artery in 5 cases. The body and the pars interarticularis of the C2 vertebra were free of the artery in all cases. The distance of the tip (or dome) of the vertebral artery loop from the midline of the C2 body, as seen from an anterior transoral surgery perspective ranged from 6.1 mm to 16.2 mm (11.7 mm). The distance of the tip (or dome) of the loop from the articular surface of the superior facet ranged from 0.6 to 4.8 mm (average 2.5 mm). The distance of the dome of the vertebral artery groove from the dome of the artery varied from 0 to 4.2 mm (average 2.7 mm). The extra space was filled up with venous plexus and periosteal tissue. In six sides (30 %) it was found that the VA artery occupied the entire volume of the vertebral artery groove in the inferior surface of the superior facet of C2. In these cases the occupancy ratio VA/bony confinements was considered to be 100%. In the remaining cases the oblique width of the bony groove, once unroofed, was measured and put in relation with the diameter of the VA in that point. The extent of the vertebral artery occupancy in the vertebral artery groove in C2 ranged from 34% to 100% (average 79 %). V2- segment:
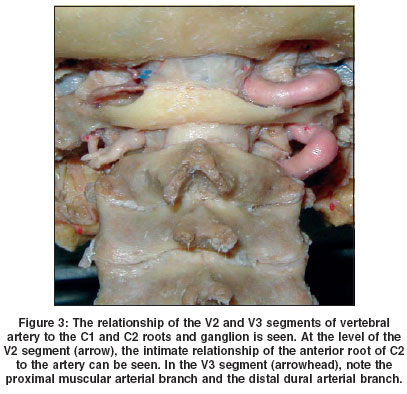
The vertebral artery exits from the transverse process of the C2 vertebra and takes an initial lateral bend and then traverses superiorly. The artery courses anterior to the two roots of the C2 ganglion. The length of this segment of the artery ranged from 12.6 mm to 32.2 mm (average 15.7 mm). The distance of the lateral edge of the ganglion from the vertebral artery ranged from 5.1 mm to 11.1 mm (average 7.5 mm). The distance of artery from the lateral end of the dural tube ranged from 14.7 mm to 17.9 mm (average 15.3 mm). Two sets of branches arise from the vertebral artery in this segment, a relatively large muscular branch and a small artery traversing along the C2 ganglion into the spinal canal. V3 segment:
After exiting the transverse process foramen of C1, the vertebral artery takes an approximately 90° posterior bend and turns medially to engage in the groove on the superior surface of the posterior arch of the atlas, where turning around the superior facet of the atlas it bends anteriorly to enter the spinal canal. The total length of this segment of the artery was 32.3 mm to 43.5 mm (average 35.7 mm). The C1 roots course posterior-inferior in relationship to the artery. The posterior inferior cerebellar artery did not arise from the segment in any specimen. The distance between the most medial extension of the vertebral artery and the medial edge of the vertebral artery groove on the outer cortex of the posterior arch of the atlas ranged from 2.1 mm to 5.2 mm (average 4.24 mm).
The vertebral artery occupancy ratio was calculated by putting in relation the width of the bony groove with the width of the artery in that point. The width of the bony groove was measured from the posterior aspect of the lateral mass of C1 to a line connecting the most medial edges of the groove on the posterior arch. The vertebral artery occupancy on the posterior arch of the atlas ranged from 42% to 71 % (average 57%).
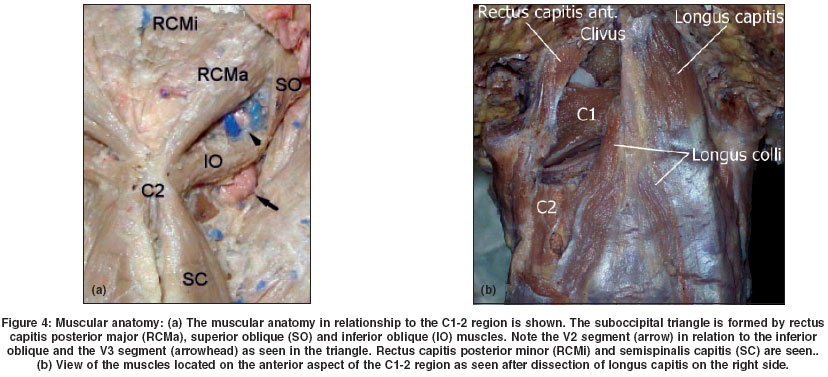
Muscular anatomy [Figure - 4]: The muscles involved with the C1-C2 complex on the anterior aspect are the recti capitis anterior and lateralis, both stretching from the anterior aspect of the transverse process of C1 respectively, to the inferior surface of the basilar occipital bone. Longus capitis extends from the inferior surface of the basilar occipital bone and clivus to its attachment on the transverse processes of the third to sixth cervical vertebrae. Longus colli is placed anterior to the vertebral column and covered by longus capitis in its superior aspect. It is divided in three parts and attaches to the transverse processes of the cervical and first thoracic vertebrae, as well as to the anterior aspect of the bodies of the first thoracic vertebrae.
On the posterior aspect the short and thick bifid spinous process of C2 gives attachment to three muscles: semispinalis cervicis extending from the second to fifth cervical spines to the transverse processes of the upper five or six thoracic vertebrae; inferior oblique, which extends to the transverse process of C1 and forms the inferior limit of the suboccipital triangle and rectus capitis posterior major, which extends to the inferior nuchal line forming the medial limit of the suboccipital triangle. The lateral limit of the triangle is formed by superior oblique, which extends from the transverse process of C1 to the inferior nuchal line. Rectus capitis posterior minor converging from the inferior nuchal line to the posterior tubercle on the arch of C1 is the only muscle that attaches to the posterior arch of the atlas. Laterally scalenus medius attaches to the transverse process of the axis and levator scapulae to the transverse process of the atlas. Discussion The C1 and C2 vertebrae are called ′atypical vertebrae′ and have unusual shape and architecture and a clinically complex and important vertebral artery relationship. Various authors have written about the danger of injury to the vertebral artery during surgery in this region.[4],[6],[7],[8],[9],[10] The popularity of transoral surgical route, lateral mass screw fixation procedures and lateral approaches to the anterior foramen magnum lesions has made learning of anatomy of the vertebral artery more relevant. The injury to the artery during surgery can lead to catastrophic intra-operative bleeding and compromise to the blood flow can lead to unpredictable neurological deficits, which will depend on the adequacy of blood flow from the contralateral vertebral artery. We could not locate any paper in the neurosurgery literature focussing on the anatomy of the vertebral artery in this region.
The vertebral artery adopts a serpentine course in relationship to the craniovertebral region. The artery has multiple loops and an intimate relationship with the atlas and axis bones. We observed a wide variability of the course of the artery in our specimens. Of the twenty vertebral arteries studied, no two arteries matched exactly in their course, in their length and in their sizes. Also the shape, size and location of the vertebral artery groove on the inferior aspect of the superior articular facet of the C2 and over the posterior arch of the atlas had wide variations. Venous plexuses covered the entire course of the vertebral artery, making identification possible during the surgery.
After a relatively linear ascent of the vertebral artery in the foramen transversarium of C6-to C3, the artery makes a loop medially towards an anteriorly placed superior articular facet of the C2 vertebra, making a deep groove on its inferior surface. The extent of medial extension of the loop varied. The distance of the artery from the midline of the vertebral body of C2 as would be observed during a transoral surgical procedure was on an average 11.7 mm. The anterior surface of the body of the C2 was continuous with the anterior surface of the superior facets on both sides with no definite identification landmark. This suggests that during transoral surgery and drilling of the C2 body, exact identification of the midline is crucial and the lateral limit of bone removal should take into account the location of the artery. The vertebral artery loops away from the midline underneath the superior articular facet of the C2. This makes drilling safe, as regards the vertebral artery, above the level of the C2 vertebral body and over the odontoid process.
Gottlieb measured superior articular facets of thirty human C1 vertebrae and found that classically described kidney shaped facet is an infrequent finding and none of the facets of the two sides were mirror images in their symmetry.[11] Huggare and Houghton analyzed articular masses of C1 in prehistoric Polynesian and Thai skeletons and observed that right-sided articular mass was constantly and significantly higher than that on the left side.[9] In the present study, we found kidney shaped superior facets in 24% facets and none of the facet had mirror symmetry.
Superior facet of C2 vertebra differs from the facets of all other vertebrae in two important characters, which make this region prone to vertebral artery injury during screw fixation. First is that the superior facet of C2 is present in proximity to the body when compared to other facets which are located in proximity to the lamina. The second is that the vertebral artery foramen is present partially or completely in the inferior of the superior facet of C2, while in other cervical vertebrae, vertebral artery foramen is located entirely in relationship with the transverse process. The pedicle of the C2 vertebra[3],[12] is relatively small. The course of the vertebral artery in relationship to the inferior of the superior articular facet of the C2 makes its susceptible to injury during transarticular and inter-articular screw implantation techniques. Various authors have cautioned against injury to the artery during the screw implantation. Paramore et al suggested that approximately 20% of the cases are not suitable for a lateral screw implantation. It was observed that the screw implantation in the superior facet of the C2 vertebra has to be sharply medial and directed towards the anterior tubercle of the C1 for trans-articular fixation[13],[14] and towards the vertebral body of C2 for interarticular fixation.[15] As discussed in our previous paper on this subject,[2] the pars-interarticularis can be divided into nine quadrants. The superior and medial compartment can be used for inter-articular technique of screw implantation. The average distance of the artery from the ganglion was 7.5 mm. It suggests that the dissection around the lateral end of the ganglion should be carefully done and under vision. The V2 segment of the artery is closest to the C1-2 joint near the inferior facet of the C1.
The vertebral artery takes a loop after its exit from the foramen transversarium of C1 vertebra. It then occupies a vertebral artery groove over the superior surface of the posterior arch of the atlas. Vertebral artery in its location over the lateral aspect of the posterior arch of the atlas is vulnerable to injury during a posterior midline approach. Ebraheim et al[8] observed that the dissection on the posterior aspect of the posterior ring should remain within 12 mm lateral to the midline, and dissection on the superior aspect of the posterior ring should remain within 8 mm of the midline. We observed that the vertebral artery groove was on an average 18.2 mm away from the midline and the vertebral artery in relationship with the groove was 22.1 mm away from the midline. The C1 roots travel inferiorly and posterior in relationship to the vertebral artery during its course over the posterior arch of the atlas. The suboccipital triangle formed by rectus capitis posterior major, inferior oblique and superior oblique muscles, helps in the identification of the vertebral artery.
It was observed that the vertebral artery did not occupy the entire vertebral artery groove on the inferior surface of the superior articular facet and over the posterior arch of the atlas. It suggests that the only bone windows of the computerised tomography are not sufficient to assess the location of the artery. Paramore et al have also observed the fact that the vertebral artery might not occupy completely the vertebral artery groove in relationship to the C2 facet.[14] We observed that the artery occupied on an average 79% of the vertebral artery groove on the inferior surface of the superior articular facet of C2 and about 57% of the vertebral artery groove over the lateral part of the posterior arch of the atlas. The multiple loops of the vertebral artery and the buffer space of the artery in the bony grooves suggests a dynamic nature of the relationship of the artery with the groove and the possibility of the changes in the location of the artery during the neck movements. It may be that the occupancy of the vertebral artery groove could change with the age. The old age of some specimens examined and the reduced elasticity of the arteries could have resulted in the reduction of the occupancy rate. The relatively ′tight′ situation of the vertebral artery where the venous buffer space was less prominent [Figure - 1]d as compared to a ′loose′ vertebral artery with significant buffer space [Figure - 2] could also play a role in the symptom of giddiness on extreme neck movement.
References
| 1. | Goel A, Desai KI, Muzumdar DP: Atlantoaxial fixation using plate and screw method: A report of 160 treated patients. Neurosurgery 2002;51:1351-7. Back to cited text no. 1 |
| 2. | Gupta S, Goel A: Quantitative anatomy of the lateral masses of the atlas and axis vertebrae. Neurol India 2000;48:120-5. Back to cited text no. 2 |
| 3. | Benzel EC: Anatomic consideration of C2 pedicle screw placement. Spine 1996;21:2301-2. Back to cited text no. 3 |
| 4. | Doherty BJ, Heggeness MH: Quantitative anatomy of the second cervical vertebra. Spine 1995;20:513-7. Back to cited text no. 4 |
| 5. | Gray H: Anatomy of the human body. 17th (Ed). Philadelphia: Lea & Febiger 1959. Back to cited text no. 5 |
| 6. | Rongming Xu, Matthew M. Nadaud, Nabil A. Ebraheim, Richard A. Yeasting: Morphology of the second cervical vertebra and the posterior projection of the C2 pedicle axis. Spine 1995;20:259-63. Back to cited text no. 6 |
| 7. | Doherty BJ, Heggeness MH: The quantitative anatomy of the atlas. Spine 1994;19:2497-500. Back to cited text no. 7 |
| 8. | Ebraheim NA, Xu R, Ahmad M: The quantitative anatomy of the vertebral artery groove of the atlas and its relation to the posterior atlantoaxial approach. Spine 1998;23:320-3. Back to cited text no. 8 |
| 9. | Huggare J, Houghton P: Asymmetry in the human skeleton. A study on prehistoric Polynesian and Thais. Eur J Morphol 1995;33:3-14. Back to cited text no. 9 |
| 10. | Xu R, Naudad MC, Ebraheim NA: Morphology of the second cervical vertebra and the posterior projection of the C2 pedicle axis. Spine 1995;20:259-63. Back to cited text no. 10 |
| 11. | Gottlieb MS: Absence of symmetry in superior articular facets on the first cervical vertebrae in humans. J Manipulative Physiol Ther 1994;17:314-20. Back to cited text no. 11 |
| 12. | Heggeness MH, Doherty BJ: The trabecular anatomy of the axis. Spine 1993;18:1945-9. Back to cited text no. 12 |
| 13. | Magerl F, Seemann PS: Stable posterior fusion of the atlas and axis by transarticular screw fixation, in Kehr P, Weidman A (Ed): Cervical Spine I. Berlin: Springer-Verlag 1987:322-6. Back to cited text no. 13 |
| 14. | Paramore GP, Dickman CA, Sonntag VKH: The anatomical suitability of the C1-C2 complex for transarticular screw fixation. J Neurosurg 1996;85:221-4. Back to cited text no. 14 |
| 15. | Goel A, Laheri V: Plate and screw fixation for atlanto-axial subluxation. Acta Neurochir (Wien) 1994;129:47-53. Back to cited text no. 15 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04055f5.jpg]
[ni04055f4.jpg]
[ni04055f3.jpg]
[ni04055f1.jpg]
[ni04055f2.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}