 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 194-196 Original Article Tuberculous meningitis with pulmonary miliary tuberculosis: A clinicoradiological study Kalita J, Misra UK Department of Neurology, Sanjay Gandhi PGIMS, Lucknow
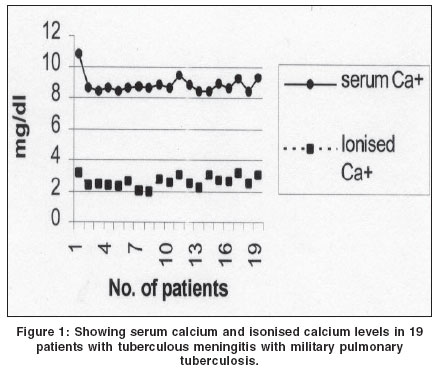
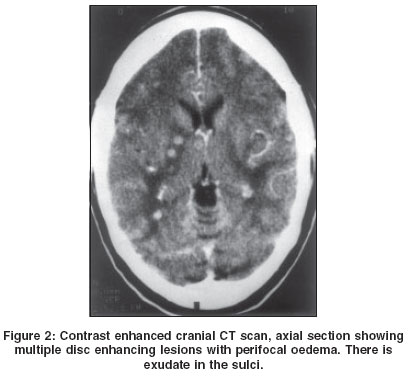
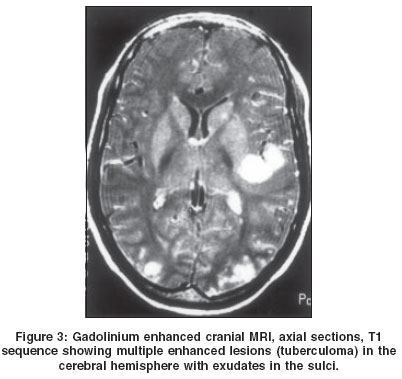
Correspondence Address:Department of Neurology, Sanjay Gandhi Post Graduate Institute of Medical Sciences, Raebareily Road, Lucknow - 226014 Code Number: ni04059 Abstract BACKGROUND AND AIMS: This study aims at evaluating the clinical and radiological outcome of tuberculous meningitis (TBM) patients with pulmonary miliary tuberculosis. MATERIAL AND METHODS: Diagnosis of TBM was based on clinical, CT scan or MRI and CSF criteria, and that of miliary tuberculosis on chest radiograph. Detailed clinical evaluation was done in all. Severity of meningitis was graded into Grades I, II and III. Complete hemogram, serum chemistry and Montaux tests were performed. The recovery was defined on the basis of 6 months Barthel index score as poor, partial or complete. RESULTS: 20 out of 165 patients with TBM had pulmonary miliary tuberculosis. Their mean age was 30 years; there was one child and 13 patients were females. The mean duration of symptoms was 6.3 months. Montoux test was negative in 9 patients. Six patients were in stage I, 3 in stage II, and 11 in stage III meningitis. Hemoglobin was below 12 gm% in 13 and liver dysfunction and hypocalcaemia was present in 8 and 18 patients respectively. CT scan was abnormal in 16 patients and revealed hydrocephalus (10), granuloma (7), exudates (3) and infarction (1). MRI was abnormal in 7 out of 8 patients and 3 of these patients had normal CT scan. MRI revealed multiple granuloma in 7 patients and exudates in 2. At 6 months, 2 patients died, 10 had complete, 2 had partial and 4 had poor recovery. CONCLUSION: TBM with pulmonary miliary tuberculosis was commoner amongst females who were anemic and hypocalcaemic. MRI revealed multiple granuloma and the majority of the patients improved. Keywords: Meningitis, tuberculous, miliary, CT, MRI, hypocalcaemia Introduction Miliary tuberculosis in immunocompetent adults is rare even in endemic areas. Data from CDC reported 1.3% cases of tuberculosis as miliary.[1] Central nervous system involvement in the form of meningitis or tuberculoma is recognized clinically in 16-30% patients with miliary tuberculosis[2],[3],[4] although meningeal involvement can be found in the postmortem in 29-54% patients.[2],[3] Most of the earlier studies on TBM with pulmonary miliary tuberculosis were conducted before the advent of modern chemotherapeutic agents and imaging.[5] Silent intracranial tuberculoma in miliary tuberculosis has been reported on gadolinium enhanced MRI.[6],[7] There is a paucity of comprehensive reports analyzing the clinical, radiological and prognosis of TBM patients with miliary pulmonary tuberculosis in the modern era. This study aims at evaluating the clinical, and CT and MRI changes in TBM patients with miliary pulmonary tuberculosis and their 6-month outcome. Material and Methods This is a retrospective analysis of 20 out of 165 TBM patients who had miliary tuberculosis of lung and who were managed in the last 8 years. They were subjected to detailed clinical evaluation. Glasgow coma scale was used for assessment of consciousness. Montaux test, hematology, serum chemistry and radiograph of chest were carried out. Contrast enhanced cranial CT scan was done using a third generation CT scanner and 10 mm axial sections were obtained. Cranial MRI was carried out on a 2T scanner operating at 1.5 T and T1, T2, PD and gadolinium enhanced T1 sequences were obtained. The presence of hydrocephalus, exudate, infarction and tuberculoma was noted. The diagnosis of TBM was based on clinical, CSF and radiological criteria. The essential criteria included presence of meningitic syndrome comprising headache, vomiting and fever for 2 weeks or more in whom malaria, septic and fungal meningitis were excluded. The supportive criteria included predominant lymphocytic pleocytosis with raised protein; radiological evidence of tuberculosis on CT or MRI scan which included exudate, hydrocephalus, tuberculoma and infarction singly or in combination, evidence of extra CNS tuberculosis and response to antitubercular therapy. The presence of essential and at least 3 out of 4 supportive criteria was considered suggestive of TBM. The presence of AFB in CSF, positive PCR, positive IgM ELISA or AFB in CSF culture was considered as definite evidence of TBM.[8] The severity of meningitis was graded into: stage I (meningitis only) stage II (meningitis with focal neurological deficit) and stage III (meningitis with altered sensorium). Patients were prescribed 4-drug antitubercular therapy (RHZE). Routine CT scan or ultrasound of abdomen, and bone marrow examination were not performed for documenting the dissemination. The outcome was defined on the basis of 6 months Barthel index (BI) score as complete (BI 20), partial (BI 12-19) or poor (BI<12).[9] Results Twenty patients with TBM had pulmonary miliary tuberculosis. Their mean age was 30 (range 10-70) years; they included one child and 13 females. The duration of symptoms ranged between 2 and 24 (mean 5.3) months. All had meningeal symptoms and signs, except fever, headache and vomiting were absent in 1, 4 and 6 patients respectively. Anorexia and weight loss were present in all except 2 patients. History of tubercular contact, alcohol addiction and recurrent skin infection was present in one each. BCG vaccination was received only by a 10-year-old child. The sensorium was altered in 11 patients and GCS score ranged between 4 and 15 (mean 13.5). Seizures were present in 7 and focal weakness in 9 (2 paraparesis, 4 hemiparesis and 3 quadriparesis). Tendon reflexes were exaggerated in 6 patients. Sensations were abnormal in the lower limbs in 2 patients who had paraplegia and 1 hemiplegic patient had hemisensory loss. Papilledema and optic atrophy were present in 3 patients each. Six patients had sixth and 4 had facial nerve palsy. Six patients were in stage I, 3 in stage II and 11 in stage III meningitis. Leucocytosis was present in 3, raised ESR in 17 and hemoglobin was below 12 gm/dl in 13 patients. Serum bilirubin was raised in 6 and transaminases were raised in 8 patients. Serum calcium ranged between 8.4 and 10.8 (mean 8.8) mg/dl and in 18 patients it was below 9 mg/dl. Serum phosphorous was normal in all but serum alkaline phosphatase was raised in 13 patients. Ionized calcium was low in all the patients (range 1.96-3.22, mean 2.60 mg/dl) [Figure - 1]. Serum protein was low in 6 patients (below 6 gm/dl) and hypoalbuminemia was present in 15 patients (below 3.5 gm/dl). Montaux test was negative in 9 patients. CSF was abnormal in all and revealed raised protein 75-400 (mean 130) mg/dl, sugar 20-60 (mean 30.2) mg/dl, and lymphocytic pleocytosis (10-300/mm3, mean 93/mm3). CSF was positive for AFB in 6, for PCR in 3 and for IgM ELISA in 1 patient. CD4+ count done in 1 patient was 145/mm3 and HIV serology was negative in all. Cranial CT scan was abnormal in 16 patients, and revealed hydrocephalus in 10 (communicating 8 and obstructive 2), periventricular cap in 3 and tuberculoma in 7 patients (single 2 and multiple 4). Meningeal enhancement was present in 3 and subcortical infarctions in 1 patient [Figure - 2]. Cranial MRI in 8 patients revealed abnormality in 7 which included multiple tuberculoma in 7 [Figure - 3] and meningeal enhancement in 2. In 3 of these patients CT scans were normal. Spinal MRI was carried out in 3 patients and revealed intramedullary cervical tuberculoma in 1, T2 hyperintensity in cervical spinal cord, and collapse of L5 vertebra in 1 each. Two patients died in the hospital. At 6-month follow-up 10 patients had complete, 2 had partial and 4 had poor recovery. One patient initially recovered completely, but developed quadriplegia at 6 months due to Pott′s spine and two were lost to follow-up. Discussion In this study on 20 TBM patients with miliary tuberculosis, 19 were adults, all belonged to a tubercular endemic area and three had a history of tuberculosis. Therefore, miliary tuberculosis in these patients was most likely of the reactivation type. None of our patients presented with pulmonary or hepatic symptomatology, although 6 patients had raised bilirubin and 8 had raised transaminases suggesting associated hepatic dysfunction. The determinants of successful dissemination include the state of specific or non-specific host cellular immunity, mycobacterial virulence and bacterial load. Our patients neither had HIV infection nor an apparent cause of immunosuppression but detailed immunological studies were not done. Negative Montaux test in 9 and low CD4 in 1 patient suggest impaired cellular immunity. Another patient was alcoholic and 1 had recurrent skin infection which may be consistent with underlying immunodeficiency. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04059f2.jpg] [ni04059f1.jpg] [ni04059f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}