 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
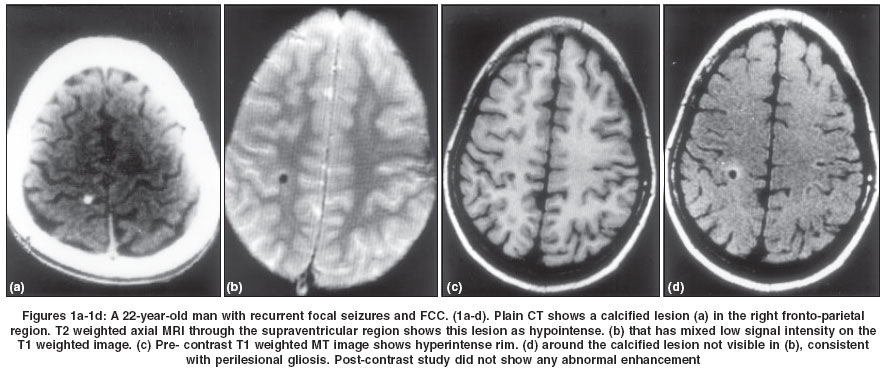
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 197-199 Original Article Epilepsy with focal cerebral calcification: Role of magnetization transfer MR imaging Agarwal Atul , Raghav Sanjay , Husain Mazhar , Kumar Rajesh , Gupta Rakesh K Department of Neurology, CSM Medical University, Lucknow
Correspondence Address:Department of Neurology, CSM Medical University, Lucknow - 226003 Code Number: ni04060 Abstract BACKGROUND: Some patients with focal cerebral calcification (FCC) have no seizure or a benign course of epilepsy, whilst others with a similar lesion have uncontrolled epilepsy. AIMS: To look for perilesional hyperintensity, presumed to be indicative of gliosis, around FCC on magnetization transfer (MT) MRI and to correlate seizure outcome with its presence. SETTING AND DESIGN: Case control study. MATERIAL AND METHODS: Fifty-one patients with epilepsy and 30 controls with single calcified cerebral lesion on CT were studied. Clinical and treatment details were noted. EEG and T1, T2, MT and contrast enhanced MRI were done. STATISTICAL ANALYSIS USED: Student's t test. RESULTS: On MT MRI, perilesional gliosis was seen around the focal calcified lesion in 17 (33.3%) patients. None of the controls had perilesional gliosis. The mean monthly seizure frequency was significantly higher in the 17 patients having perilesional gliosis (2.63+1.15) as compared to the 34 patients without it (0.59+0.63; P= 0.0014). Perilesional gliosis was seen in 8 out of 11 (72.7%) patients who were on 2 AEDs and in all 5 (100%) patients who were on 3 or more AEDs. It was present only in 4 (11.4%) out of 35 patients who were on one AED. CONCLUSION: Gliosis around a cerebral calcified lesion as seen on T1 weighted MT MRI indicates poor seizure control.Keywords: Neurocysticercosis, focal cerebral calcification, cysticercus granuloma, gliosis, seizure Introduction Cranial computed tomography (CT) in patients with partial seizures with or without secondary generalization often reveals single or multiple small (< 10 mm) calcified lesions labeled as focal cerebral calcifications (FCCs).[1],[2] The most common etiology of FCC is cysticercosis. Other causes of FCC include healed tuberculoma, fungal granuloma or small calcified AV malformation.[1],[3],[4] About 16% to 45% of cysticercosis granuloma end up as calcification.[4],[5],[6] The prognosis of seizures is worse if the lesions calcify as compared to those showing complete resolution.[7],[8],[9] Even in patients with FCC-related epilepsy some have a benign course while others have multiple seizures which may be difficult to control even with anti-epileptic drugs (AEDs). Magnetic resonance imaging (MRI) has been used to study the characteristics of these lesions.
Magnetization transfer (MT) MRI, a relatively new addition in this field, modifies image contrast using an off-resonance saturation selective pulse to saturate protons associated with macromolecules.[10] The technique is useful in the characterization of tumors, infections, trauma and other white matter abnormalities.[11] Recently, it has been reported that perilesional abnormality seen on T1 weighted MT images, which is presumed to be gliosis, correlates with the course of seizures and the ultimate prognosis in patients with neurocysticercosis-related epilepsy.[6],[12] Material and Methods A total of 51 consecutive patients of epilepsy (27 males and 24 females; age range 7 to 37 years; mean 17.3 ± 8.4) were studied from July 1999 to December 2001. The inclusion criteria were: (i) a single calcified CT lesion without perilesional edema, and (ii) duration of epilepsy of more than one year with at least one seizure in the previous six months while on AEDs. Those patients who had more than one calcified lesion and those with non-compliance to their treatment were excluded. These patients were already on AED treatment for their epilepsy management for at least one year under the care of a neurologist. Detailed history was taken emphasizing duration of epilepsy, type of seizures, AED given and their doses. Seizure types were recorded as per the descriptions given by the patient, relatives and/or nearest kin. Monthly seizure frequency for the previous six months was noted. Thirty-five patients were on 1 AED [20 on carbamazepine (CBZ), 11 on phenytoin (PHT) and 2 each on phenobarbitone (PB) and valproate (VPA)]. Eleven patients were on 2 AEDs (CBZ and VPA = 5, CBZ and clobazam = 3, VPA and PHT = 2, and PHT and PB = 1). Four patients were on 3 AEDs and one patient was on 4 AEDs. The blood levels of AEDs were not estimated due to financial constraints. Thirty individuals with a single calcified brain lesion on CT with no19.03.04 history of seizures were included as controls. There were 14 males and 16 females, age ranging from 11 to 45 (mean 22.5 ± 6.5) years. Twenty-four presented with chronic tension type headache and 6 had depression. Ethical clearance was taken from the local review board and informed consent was taken from all the patients or caregivers and controls. All the patients and controls had one or more inter-ictal awake EEGs on 21 channels Nihon Kohden machine (Neurofax 441-A / year 1990). Cranial MRI was done on a 1.5 T superconducting system (Magnetom SP 63/85, Siemens, Erlangen, Germany) using a circular polarized head coil. Conventional Spin Echo (CSE) proton density, T1, T2 weighted and T1 weighted magnetization transfer spin echo (MTSE) MRI was performed.[6] Phase-corrected gradient echo (GRE) imaging was also done in some patients. Post-contrast T1 weighted MT imaging was performed using gadolinium-DTPA at a dose of 0.1 mmol/kg of body weight intravenously. Other than a recent CT scan showing a solitary calcific lesion, 20 patients also had with them initial CT done one to five years earlier (mean 16.4 ± 9.8 months), which showed a solitary lesion suggestive of cysticercosis at the same site as that of the present calcification. Demonstration of scolex on phase-corrected GRE imaging confirmed this etiology in 14 patients.13 In the remaining 17 patients and all controls, we presume the etiology of calcified lesions to be healed cysticercosis due to its regional endemicity. Immunological tests for cysticercosis were not planned as it has been shown to have low sensitivity in a single cysticercus lesion.14 All images were analyzed (by RKG and RK) for the presence of perilesional gliosis. Perilesional gliosis was considered to be present when perilesional hyperintensity was seen on T1 weighted MT images with no visible abnormality on T2 weighted images and the perilesional MT ratio was lower than that of the contralateral normal brain.6,15 Data was analyzed by SPSS software (version 9.0) using student′s t-test to look at the relationship of gliosis with seizure frequency. Results The duration of epilepsy in these patients with FCC ranged from 1 to 10 years (mean 4.5 ± 2.4 years). Thirty-four (66.6%) patients had partial seizures (simple n=22, 64.7%; complex n=12, 35.2%) while 8 (15.6%) had secondary generalized seizures. Nine (17.6%) patients had only generalized tonic clonic seizures. Out of 42 patients who had partial seizures with or without secondary generalization, the site of FCC corresponded to the semiology of seizures in 28 patients. In 20 patients, the past presentation was of acute symptomatic epilepsy due to cysticercal lesion and later the lesion calcified resulting in remote symptomatic epilepsy. Seizure frequency was variable and ranged from one per 6 months (0.17 per month) to 4 per month with mean being 1.27 ± 0.51 per month in the preceding 6-month period. Inter-ictal awake EEGs were abnormal in 18 (35.2%) patients, showing focal spikes or sharp waves in 8 patients and focal slow waves in 10 patients. Focal abnormalities in the majority (14/18) correlated with the site of the calcified lesion. In the control group, 26 individuals had normal EEGs, 2 had non-specific generalized slowing, while another 2 had generalized beta activity. Parietal FCC was most common (n=24, 47%), while occipital, frontal and temporal lesions were seen in 15, 10 and 2 patients respectively. In the controls, the distribution of FCCs was: parietal (n=12), frontal (n=9), occipital (n=6) and temporal (n=3). On T1 weighted MT images, the presumed gliosis around FCC was seen in 17 (33.3%) out of 51 patients [Figure - 1]. No perilesional gliosis was seen in any of the controls. The MT ratio value in hyperintense perilesional regions was 21.9 ± 2.4 while in the corresponding normal contralateral regions it was 28.75 ± 1.07, (P=0.012). There was no evidence of abnormal contrast enhancement in any of the patients or controls. On the basis of the perilesional gliosis demonstrated on T1 weighted MT MRI, the patients were divided into 2 subgroups i.e. the one with gliosis (Group A) and the other without gliosis (Group B). The duration of the epilepsy was not statistically different in the two groups (4.8 ± 2.6 vs. 4.35 ± 2.2 years, p=0.16). The mean monthly seizure frequency in the 17 patients of Group A was significantly higher (2.63 ± 1.15) as compared to that of the 34 patients of Group B (0.59 ± 0.63 P = 0.0014). Out of the 35 patients who were being managed on single AED, gliosis was present only in 4 (11.4%) patients, while 8 out of 11 (72.7%) patients who were on 2 AEDs and all the 5 patients on 3 or more AEDs had perilesional gliosis. Out of 17 patients who had perilesional gliosis, 10 had abnormal EEG in comparison to only 8 out of 34 patients without gliosis. No patients with refractory epilepsy could be taken up for epilepsy surgery. Discussion In this study we evaluated 51 patients of active epilepsy with single FCC. No perilesional hyperintensity on T1 weighted MT images suggestive of gliosis was seen around FCCs of 30 controls who never had epilepsy while it was seen around one-third of FCCs with active epilepsy. Those patients who had perilesional gliosis more often had abnormal EEGs and a significantly higher seizure frequency even when on AED treatment and they were often on more than one AED in comparison to those without gliosis. This suggests relative refractoriness of epilepsy to antiepileptic drug treatment probably due to perilesional gliosis. As there was no difference in the duration of epilepsy in the two groups, it is unlikely that repeated seizures contribute to the development of gliosis. Although FCC may be an asymptomatic or coincidental finding in some of the patients, often the single lesion or one or more of the multiple lesions are associated with seizure activity.[1],[2],[3],[4] In the majority of our patients with epilepsy, the FCC corresponded with the possible site of epileptogenesis. Out of 29 calcified lesions in the only other available study, perilesional gliosis was seen only in 5 (17%).[6] However in the present series, perilesional gliosis was observed more frequently (33.3%). This appears to be because one of our inclusion criteria was patients with active epilepsy with FCC. While the seizures in the setting of an actively degenerating or involuting cysticercosis are classified as acute symptomatic, those with calcified lesions are considered unprovoked. Inflammation around dead cysts has been documented in pigs16 and after treatment in humans.[5] Unless proved histologically, there may be questions regarding the exact nature of perilesional hyperintensity on T1 MT MRI which is presumed to be gliosis. A single report of the histopathological examination of FCCs and surrounding tissue is available.[17] In the immediate vicinity of the lesion, the tissue reaction consisted of astrocytic gliosis, angiogenesis, inflammatory infiltrates and a small rim of demyelination.[18] The decreased MT ratio observed in this and other studies has been attributed to increased water content in the brain tissue, damage to myelin and gliosis.[11] It appears that the residual perilesional astrogliosis remains as a sequelae of the perilesional inflammation seen in the acute stage in degenerating cysticercus that is shown as an area of low MT ratio with T1 weighted MT MRI. Once developed gliosis is likely to persist. If seizure control is unsatisfactory, there is reason to believe that lesionectomy may offer good results. The histological examination of tissue obtained surgically in future studies should provide pathological details of the abnormality. Conclusion Although calcified lesions in cysticercosis are considered as poor prognostic indicators of seizure control, not all calcified lesions are associated with a poor outcome. The presence of perilesional gliosis as seen on T1 weighted MT MRI is associated with difficult seizure control and is of value in objective prognostication of seizure outcome in these patients. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04060f1.jpg] |
| |||||||||

{kind=link}