
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 200-202
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 200-202
Original Article
A clinical study of non-parkinsonian and non-cerebellar tremor at a specialty movement disorders clinic
Shukla Garima , Behari Madhuri
Department of Neurology, All India Institute of Medical Sciences, New Delhi
Correspondence Address:Department of Neurology, Neurosciences Center, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110029
garimashukla@hotmail.com
Code Number: ni04061
Abstract
BACKGROUND: No Indian studies have focused on the clinical aspects of tremor. AIMS: To study the distribution of various etiological types of tremor disorders at a Movement Disorders clinic of a large, tertiary care hospital in India and to study the clinical characteristics of essential tremor [ET]. SETTING AND DESIGN: Prospective cross-sectional study at a tertiary care specialty clinic. MATERIAL AND METHODS: Patients presenting with tremor as the chief complaint, with no features suggestive of parkinsonism, cerebellar disorder or acute central nervous system disorder, were included. Patients were classified into different etiological categories from detailed history. All patients diagnosed as ET, were further interrogated for a detailed family history and examined for characteristics of tremor. These patients were then classified into 'definite', 'probable' and 'possible' ET. RESULTS: One hundred and six patients (mean age 44.4 + 15.1 years) were examined during the study period. ET (59.4%) and dystonic tremor (21.7%) were the commonest types. Only 43% patients of ET reported progression; response to alcohol was seen in only a single patient, a positive family history was present in 52.4% and in 36.4% the inheritance was of an autosomal dominant pattern. CONCLUSION: ET and dystonic tremor are the commonest causes of tremor presenting to a specialty Movement Disorders clinic. Most patients with ET have high-frequency tremor, with mild asymmetry in 40% cases. Alcohol responsiveness may not be a useful tool in the diagnosis of ET.
Keywords: Essential tremor, dystonic tremor, clinical diagnostic
categories
Introduction Tremor is a periodic movement about an axis, which distinguishes it from other movement disorders such as chorea, myoclonic jerks and tics which may not have a fixed period and may involve complex movements other than simple oscillations.[1] Tremor has been described as the most frequent pathologic symptom of basal ganglia disorders.[2] Prevalence estimates of ET vary from 0.008% to 22% representing a 2750-fold difference.[4],[5] The diagnosis of ET is largely clinical which contributes to this vast difference in prevalence estimates. Recently, a reliable set of diagnostic criteria, showing a high inter-observer concordance rate was published by the WHIGET group.[5],[6] The diagnosis made on using this screening questionnaire correlated closely with that made by neurological examination.[7] Such a questionnaire was contemplated to be a useful tool in screening patients of ET in crowded outpatient departments at our center and then studying these patients in detail.
We aimed to determe the distribution of various types of tremor disorders in patients presenting to the Movement Disorders clinic and to study the clinical characteristics of patients of ET among this heterogeneous group.
Material and Methods
All patients attending the Movement Disorders clinic at the All India Institute of Medical Sciences, New Delhi, India, with tremor as the only or predominant complaint, between December 1998 and September 2000 were recruited in the study. Patients with clinical features suggestive of a parkinsonian syndrome, cerebellar disorder or acute central nervous system disease and those less than 12 years in age were excluded from the study. Patients with unilateral tremor or those in whom a structural pathology was suspected were also excluded. Since this was a completely clinical study, ethical clearance was not considered necessary. Informed consent was obtained from all patients, however.
Personal and demographic particulars of all the patients were noted, including their age, gender, education and occupation. All patients included in the study were administered the screening questionnaire for ET proposed by Louis et al,[7] and a pre-formed set of questions pertaining to other common causes of tremor. Other clinical details noted were the duration of tremor, course of disease, activities inducing and aggravating it as well as relieving factors. A ′historical diagnosis′ thus arrived at was confirmed by further examination.
Accepted criteria were used to diagnose the different types of tremors.[3],[8],[9]
All patients diagnosed as ET were then interrogated for a detailed family history. Family history was considered ′definite′ when the family member with history of tremor was personally examined; it was considered ′probable′ if at least five questions from the screening questionnaire used were answered as ′yes′ for the secondary case and ′possible′ if at least three questions were answered as ′yes′. Family history was considered ′negative′ if there was no history of tremor in any of the family members or the answer "yes" was given for less than three questions. Patients with ET were then examined in detail. Tremor in each affected body part was graded on a scale of ′0′ to ′+ 4′ in different postures and on performing five activities of daily living (pouring water from a glass, using a spoon to drink water, drinking water from a glass, finger to nose test and drawing a spiral). Patients were then classified into three categories: ′definite ET′, ′probable ET′ and ′possible ET′.[5] After establishing the diagnosis of other types of tremor except ET, other details of those patients were not studied.
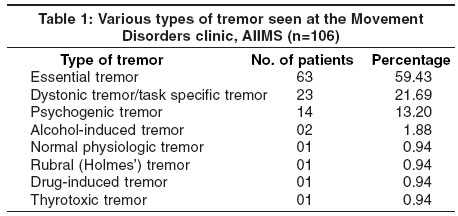
Relevant investigations were conducted in the patients according to clinical suspicion. Serum T3, T4 and TSH levels were obtained when suspicion of thyrotoxic tremor was present. Neuroimaging of the brain was planned in patients clinically suspected to have structural pathology responsible for tremor, especially in patients with unilateral limb tremor. Results One hundred and six patients (85 males) were recruited during the study period. The mean age was 44.5 ±15.1 years (range: 18 to 75 years) with the mean duration of the symptoms 5.3 ± 6.3 years (range: 15 days to 22 years). The total number of new patients of all movement disorders seen during the study period was 832. Essential tremor was the commonest type of tremor seen at our clinic, dystonic and task specific tremors being the second largest group [Table - 1]. Essential tremor patients
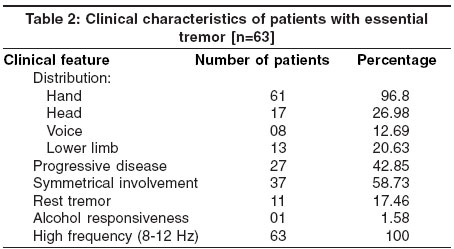
A total of 63 patients (49 males, 14 females) of ET were seen [Table - 2], with mean age of 45.8 ± 16.0 years (range: 18 to 75 years). Progression of symptoms was reported in 27 (42.9%), while the rest felt that the disorder was static. Thirty-seven patients had symmetrical involvement of both sides, the rest observed one of the sides to be worse affected. However, the difference observed in most patients was only mild. No patients had dystonia of any body part. Bilateral hand tremor, either isolated or with involvement of other body parts was seen in 61 (96.8%), head tremor in 17 patients, lower limb tremors in 13 patients, while voice tremor was observed in only 8 patients. Rest tremor was observed in 11 (17.5%) patients, though all patients had either or both of postural and kinetic tremor. High-frequency tremor was seen in all the patients. Alcohol responsiveness could be tested only in 9 patients, as the rest were teetotalers. Only one of these patients reported improvement with alcohol. All patients reported disappearance of the tremor with rest and aggravation with emotional stress.
Positive family history was found in 33 out of the 63 (52.4%) patients of ET, it was definite in 6, probable in 17 and possible in 10 patients. Three patients reported family history of Parkinson′s disease also. An autosomal dominant pattern was observed in 12 patients (36.4%), while in the rest, no conclusive inheritance pattern was observed. Dystonic Tremor patients
All 23 patients with dystonic tremor had asymmetric, multiplanar tremor, with changing frequency and amplitude in different postures. All patients had bilateral hand tremor, while 3 among these 23, had associated writer′s cramp. No patients had dystonia of other body parts. Discussion In our report, as previously described,[10] the age range was wide, but males were thrice as frequent as females. The reasons for male preponderance in India are several; women in India usually ignore symptoms, especially those which do not hamper daily activities. Long-standing tremor with positive family history is easily diagnosed by general physicians.
We classified dystonic tremor separately due to the entirely different clinical characteristics of the tremor, associated dystonia and difference in its management. The term ′dystonic tremor′ is unacceptable to some authorities on Movement Disorders as ′dystonia-associated tremor′ and ′dystonic tremor′ have often been grouped under the rubric of ET variants or simply as accompanying movement disorders. However, the Consensus Statement of the Movement Disorder Society has classified ′dystonic tremor′ as a separate entity.[3] Among the 73 patients of ET seen by Louis et al, in their community-based study, no patients had associated dystonia. This is because the diagnostic criteria proposed earlier by these authors were used for the diagnosis of ET and most of the patients with tremor in the body part affected by dystonia would have been excluded.[11] Although the commonest type of dystonia seen in previous studies, with tremor, is cervical dystonia,[12],[13] we found hand tremor (including dystonic writer′s cramp) to be the commonest in our group of dystonic tremors. This could be explained by the fact that we strictly followed the definition of dystonic tremor[3] and excluded patients who had dystonia with tremor affecting other unaffected body parts. A previous study, using a similar definition of dystonic tremor as ours, however, reported an equally high incidence of cervical dystonia in patients of dystonic tremor.[13] As these authors selected subjects from a ′dystonia clinic′, there was selection bias in the study. Most patients visiting our hospital belong to the lower socio-economic strata and these patients may not spend money and time on visiting a specialty clinic for cervical dystonia with head tremor till it becomes severe or is associated with pain. They may not visit a doctor for cosmetic reasons alone. This is confirmed by the community study of Louis et al, in which most of the patients were unconcerned about their tremor, and did not consult a doctor.[11]
We found a relatively high percentage of patients with psychogenic tremor; referral bias may again be an explanation for this occurrence, as we have a very strong Psychiatry department with exposure to movement disorders clinic. Tremor was the commonest psychogenic movement disorder in a study reporting 28 patients with psychogenic movement disorders among 842 consecutive patients with different movement disorders. Half of these 28 patients had psychogenic tremor.[14]
Few differences in the characteristics of tremor in patients with ET were observed, compared to published reports. Less than half (42%) of our patients reported lack of progression in their tremor and all had frequency of tremor in the higher range. This may be accounted for by the relatively short duration of tremor in most of our patients. High-frequency tremor seen in our patients may be partially due to the fact that our patients were younger (mean age was 45.7 years). With advancing age usually the amplitude increases and frequency decreases, thus making the tremor more disabling.[15] The reason why most of our patients did not report progression may be that the average duration of the tremor in our series was only about 5 years, thus, they may not have experienced considerable deterioration till the time they presented to us. Mild asymmetry is known in ET,[3] this was also seen in the present study. The anatomical distribution of tremor was also similar to that reported previously. The characteristic involvement of the hands with head and voice tremor with relative sparing of legs helps in differentiating severe ET from Parkinsonian tremor.[12],[16],[17] Alcohol responsiveness, considered diagnostic of ET, has been reported very commonly in patients of ET.[12],[18] This could not be assessed in our series as alcohol consumption was reported in only 9 patients, and 8 of these did not observe any major change in the tremor with alcohol. A similar observation was reported by Louis et al.[11] Family history was positive in 52.4% of ET patients in the present study, very similar to the 62.5% positivity seen in the large population of ET patients observed by Louis et al.[12] The autosomal dominant pattern was observed in only a few families, due to known variable penetration, as also due to low certainty with which many patients give the family history.
To conclude, ET is the most common cause of tremor in patients presenting to a specialty Movement Disorders clinic (59.43%), dystonic tremor being the second most common (21.69%). We observed that alcohol responsiveness could not be used as a diagnostic criterion in India, as many patients are teetotalers.
References
| 1. | Findley LJ, Cleeves L. Classification of Tremor. In: Disorders of Movement: Clinical, Pharmacological and physiological aspects. Academic Press Ltd 1989:505-19. Back to cited text no. 1 |
| 2. | Deuschl G. Editorial. Mov Disord 1998;13:1. Back to cited text no. 2 |
| 3. | Deuschl G, Bain P, Brin M. Consensus Statement of the Movement Disorder society on Tremor. Mov Disord 1998;13:2-23. Back to cited text no. 3 [PUBMED] |
| 4. | Tanner CM. Epidemiology of movement disorders. In: Anderson DW, ed. Neuroepidemiology: A tribute to Bruce Schoenberg. Boca Raton, FL: CRC Press 1991:193-216. Back to cited text no. 4 |
| 5. | Louis ED, Ford B, Lee H, Andrews H, Cameron G. Diagnostic Criteria for Essential Tremor-A Population Perspective. Arch Neurol 1998;55:823-8. Back to cited text no. 5 [PUBMED] [FULLTEXT] |
| 6. | Louis ED, Ford B, Bismuth B. Reliability between two observers using a protocol for diagnosing Essential Tremor. Mov Disord 1998;13:287-93. Back to cited text no. 6 [PUBMED] |
| 7. | Louis ED, Ford B, Lee H, Andrews H. Does a screening questionnaire for essential tremor agree with the physician's examination? Neurology 1998;50:1351-7. Back to cited text no. 7 [PUBMED] |
| 8. | Shahani BT. Tremor associated with peripheral neuropathy. In: Findley LJ, Capildeo R. (Ed). Movement Disorders: Tremor. London: Macmillan Press 1984:389-406. Back to cited text no. 8 |
| 9. | Fahn S. Atypical tremors, rare tremors and unclassified tremors. In: Findley LJ, Capildeo R, (Ed). Movement Disorders: Tremor. London: Macmillan Press 1984:431-43. Back to cited text no. 9 |
| 10. | Findley LJ, Koller WC. Essential Tremor: A review. Neurology 1987;37:1194-7. Back to cited text no. 10 [PUBMED] |
| 11. | Louis ED, Ford B, Wendt KJ, Cameron G. Clinical Characteristics of Essential Tremor: Data from a community-based study. Mov Disord 1998;13:803-8. Back to cited text no. 11 [PUBMED] |
| 12. | Lou JS, Jankovic J. Essential tremor: Clinical correlates in 350 patients. Neurology 1991;41:234-8. Back to cited text no. 12 [PUBMED] |
| 13. | Dubinsky RM, Gray CS, Koller WC. Essential tremor and dystonia. Neurology 1993;43:2382-4. Back to cited text no. 13 [PUBMED] |
| 14. | Factor SA, Podskalny GD, Molho ES. Psychogenic Movement disorders: Frequency, clinical profile and characteristics. J Neurol Neurosurg Psy 1995;59:406-12. Back to cited text no. 14 [PUBMED] |
| 15. | Elble RJ, Higgins C, Leffler K, Hughes L. Factors influencing the amplitude and frequency of essential tremor. Mov Disord 1994;9:589-96. Back to cited text no. 15 [PUBMED] |
| 16. | Rautakorpi I, Takala J, Marttila RJ, Sievers K, Rinne UK. Essential tremor in a Finnish population. Acta Neurol Scand 1982;66:58-67. Back to cited text no. 16 [PUBMED] |
| 17. | Findley LJ, Gresty MA. Tremor. Br J Hosp Med 1981;26:16-32. Back to cited text no. 17 [PUBMED] |
| 18. | Jankovic J. Essential Tremor: Clinical characteristics. Neurology 2000;54:S21-5. Back to cited text no. 18 [PUBMED] |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04061t2.jpg]
[ni04061t1.jpg]
|

{kind=link}
{kind=link}