
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 220-223
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 220-223
Original Article
Predictive value of routine hematological and biochemical parameters on 30-day fatality in acute stroke
Bhatia RS, Garg RK, Gaur SPS, Kar AM, Shukla R, Agarwal A, Verma R
Department of Neurology, King George's Medical University, Central Drug Research Institute, Lucknow
Correspondence Address:Department of Neurology, King George's Medical University, Lucknow - 226 003
garg50@yahoo.com
Code Number: ni04067
Abstract
OBJECTIVE: This prospective study was planned to study the prognostic value of routine clinical, hematological and biochemical parameters, including platelet aggregation in patients of acute stroke, on fatality occurring during the first 30 days. MATERIAL AND METHODS: In this study 116 consecutive patients (77 males and 39 females) of stroke (within 72 hours of onset) were included. After clinical evaluation and neuroimaging, blood investigations, hemoglobin, total leukocyte count, platelet count, platelet aggregation, erythrocyte sedimentation rate (ESR), blood sugar, urea, creatinine, sodium, potassium, serum cholesterol, serum bilirubin, aspartate aminotransferase (SGOT), alanine aminotransferase (SGPT), albumin, and globulin estimations were performed. The patients were followed up for a maximum period of 30 days from the onset of stroke, and patients who expired were grouped as 'expired' and the rest as 'survivors'. Logistic regression analysis was carried out among the significant parameters to identify independent predictors of 30-day fatality. RESULTS: Univariate analysis demonstrated that among hematological parameters, high total leukocyte count and ESR, at admission, correlated significantly with an undesirable outcome during the initial 30 days. Among biochemical parameters, elevated urea, creatinine, serum transaminases (SGOT and SGPT) and globulin levels correlated significantly with death. Logistic regression analysis demonstrated that a low Glasgow Coma Scale (GCS) score along with biochemical parameters such as high serum creatinine, SGPT, ESR and total leukocyte count correlated with death. CONCLUSION: Impaired consciousness, high total leukocyte count, raised ESR, elevated creatinine and SGPT levels, estimated within 24 hours of hospitalization, are the most important indicators of 30-day mortality in patients with first-time ischemic stroke.
Keywords: Stroke, intracerebral hemorrhage, cerebral infarction,
prognosis, urea, creatinine, electrolytes
Introduction The early hours after an acute stroke are crucial, because it is the most useful time for effective intervention. It is important to determine the prognostic factors as early as possible. Many studies have highlighted the prognostic importance of various laboratory parameters like blood sugar, total leukocyte count, and erythrocyte sedimentation rate (ESR).[1],[2],[3] However, few studies are available which have studied collectively the prognostic value of these parameters on multivariate analysis.[4] In this prospective study we have evaluated the significance of routine blood parameters for 30-day mortality. Material and methods
This study was conducted on patients of acute stroke admitted to the Neurology Department of King George′s Medical University, Lucknow from February 2000 to July 2001.
All patients included in the study had a clinical diagnosis of stroke supported by immediate neuroimaging. Stroke was defined, according to the WHO definition, as rapidly developing clinical signs of focal (or global) disturbance of cerebral function, lasting more than 24 hours or leading to death with no apparent cause other than of vascular origin.[5] The time of onset of the stroke was defined as the time when the patient or observer first became aware of the symptoms. All the patients who presented within 72 hours of onset, irrespective of age, sex or type of stroke, were included in the study. Patients with previous history of stroke were excluded.
After inclusion, each patient was subjected to a detailed clinical evaluation. A detailed history of risk factors of stroke was also recorded. A Glasgow coma scale (GCS) score was obtained for each patient. Apart from computed tomography (CT), blood investigations which were performed included hemoglobin, total leukocyte count, platelet count, platelet aggregation, ESR, blood sugar, urea, creatinine, sodium, potassium, and serum cholesterol. For the assessment of liver functions, bilirubin, aspartate aminotransferase (SGOT), alanine aminotransferase (SGPT), albumin, and globulin estimations were performed. Informed consent was taken for each patient. Subsequently, the patients were treated according to the standard treatment protocols of our hospital. The study in no way interfered with the treatment. The patients were followed up for a maximum period of 30 days from the onset of stroke, and patients who expired were grouped as ′expired′ and the rest as ′survivors′. Patients discharged from the hospital before this period, were asked to visit the outpatient department at weekly intervals. Those failing to turn up for weekly follow-up were inquired for outcome either telephonically or by home visit. Those patients who left against medical advice or were discharged on persistent request were excluded from the study.
Blood samples were collected immediately after admission, before starting any intravenous infusion, from anticubital vein without producing venous stasis with a 20-gauge needle in plastic disposable syringes. Blood samples were immediately sent to the laboratory for evaluation.
For platelet aggregation studies, 6.4 ml of blood was collected in 0.6ml of 3.8% of trisodium citrate in plastic tubes, the morning after admission. Samples were sent to the Central Drug Research Institute, Lucknow and analyses were performed within one hour of collection. In patients with cerebral ischemia antiplatelet drugs and other antithrombotic therapy were started only after collecting the required blood samples.
The hematological and biochemical investigations were carried out in the hematology and biochemistry laboratories of our hospital, using standard commercial reagent kits.
The citrated blood samples were kept at room temperature for 15 minutes and then centrifuged at 100G for 10 minutes to obtain platelet rich plasma (PRP). The PRP was transferred to plastic tubes by autopippettes. The remaining blood was further centrifuged for 10 minutes at 1000G to obtain platelet poor plasma (PPP). Subsequently, ADP-induced aggregometry was performed at 37°C according to the turbidimetric method of Born with the use of an automated dual chambers aggregometer (Aggrecorder PA 3210 Kyoto Daichi, Kagaku Co. Ltd., Japan). Peak platelet aggregation in 10 minutes was recorded.
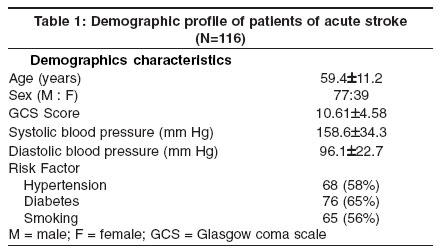
The results so obtained were recorded and analyzed by the student ′t′ test and by univariate analysis. Multiple logistic regression analysis was done for parameters found significant in univariate analysis.Results A total of 148 patients of stroke were admitted during the study period. Out of these, 8 patients were excluded because of past history of stroke. Twelve patients were excluded because they presented more than 72 hours after the onset. One hundred and twenty-eight patients were enrolled but in 12 patients, the end point could not be measured because of inadequate follow-up and hence were excluded from the study. A total of 116 patients were included (77 males and 39 females).
The demographic characteristics of all 116 patients are summarized in [Table - 1]. Sixty-two per cent (30 out of 48) patients with intracerebral hemorrhage expired whereas 22 % (15 of 68) patients with cerebral infarction expired. The mean duration of hospital stay in expired patients was shorter (5.4 ± 4.6 days) as compared to survivors (12.4 ± 8.4 days). The mean GCS score at admission was significantly lower in expired patients (6.4±3.5) as compared to survivors (13.1±2.9).
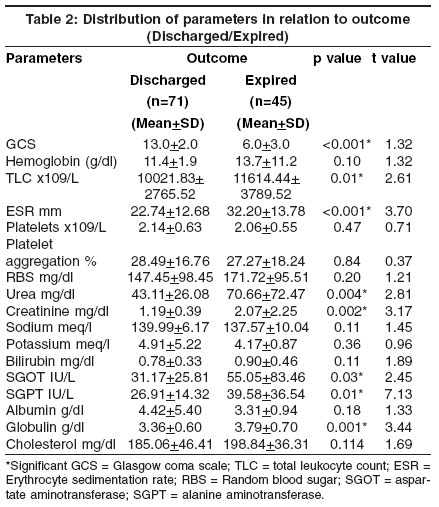
As shown in [Table - 2], after univariate analysis, amongst hematological parameters, high total leukocyte count and ESR, at admission, correlated significantly with undesirable outcome. None of the other hematological parameters studied (hemoglobin, platelet count and peak platelet aggregation) had any significant statistical correlation with regards to the outcome. Amongst the biochemical parameters, elevated urea, creatinine, serum transaminases (SGOT and SGPT) and globulin levels correlated significantly with death. Other biochemical parameters (random blood sugar, sodium, potassium, bilirubin albumin and cholesterol) did not differ significantly in the survivors and expired patients.
Logistic regression analysis was carried out amongst the significant parameters to identify independent predictors of 30-day fatality in acute stroke [Table - 3]. A low GCS score was also included in the model and was found to be significantly lower in the expired patients. High serum creatinine, SGPT, ESR and total leukocyte count correlated with death. Discussion In this study the prognostic value of various routine clinical and biochemical parameters has been evaluated. The only clinical parameter evaluated in our study was the GCS score to quantify the level of consciousness. Like several studies in the past,[5],[6] our study also suggested that a low GCS score was predictive of poor outcome.
Possibly, changes in hematological parameters at the onset of stroke play an important role in altering the cerebral blood flow.[3],[4],[7] Czlonkowska et al[4] demonstrated the importance of hematocrit as a predictive factor of 30-day fatality.[4] In our study, hemoglobin, platelet counts and platelet aggregation analysis did not show any significant difference amongst expired patients and survivors. In another study, platelet count obtained within 48 hours was significantly lower in patients of ischemic stroke than the control group. The platelet count was also significantly lower in patients who later expired than who survived.[8] Leukocytosis also influences the prognosis. Several mechanisms by which leukocytes may be implicated in parenchymal brain injury include vessel plugging, release of hydrolytic enzymes, oxygen free radicals or initiation of thrombosis.[9] Leukocytosis might also be a manifestation of some common causes of fever (e.g., pulmonary or urinary tract infections, sepsis, or pulmonary embolism from deep vein thrombosis). Czlonkowska et al[4] have also demonstrated leukocytes as an independent predictor of 30-day case fatality in stroke patients. In our study, total leukocyte counts were significantly higher in expired patients, both on univariate and multivariate analysis. A high ESR value has been associated with large ischemic lesions and more severe deficits.[3] An elevated ESR value may indicate a greater increase in the concentration of fibrinogen; a more pronounced reduction in the cerebral blood flow, a larger lesion and a poor outcome.[10] Like other studies in the past, [4] in our study, a high ESR was associated with a poor prognosis.
Elevated blood glucose has been implicated as a poor prognostic factor for cerebral ischemia and hemorrhage.[11] Animal studies have demonstrated the aggravation of ischemic injury by hyperglycemia.[12] Diabetes predisposes to occlusive vascular disease but not to intracerebral hemorrhage.[13] However, in hemorrhagic strokes it predisposes to larger size of hematoma and increased mortality at 30 days.[14],[15] In diabetics, ischemic strokes are often associated with large infarct size and poor outcome due to decreased autoregulation and changes in blood coagulability.[13] Even in non-diabetic patients with hyperglycemia, the size of the lesion and neurological deficit were worse.[16] Many studies deny the prognostic significance of elevated blood glucose.[17],[18] Our study also did not observe prognostic significance of blood sugar. In our series, on univariate analysis, blood urea and creatinine levels were found significantly higher in patients who later expired. High creatinine significantly affected poor outcome on multivariate analysis. No independent effect of urea was noted on mortality. Woo et al have demonstrated that higher plasma urea and creatinine levels are associated with more severe stroke and a low GCS score, however, these parameters have no independent effect on mortality. [18] We could not observe any prognostic value of electrolyte estimations. Among liver function tests serum transaminases and globulin levels were found to be significantly associated with poor outcome on univariate analysis. After multivariate analysis, only SGPT correlated with poor outcome. Low albumin levels were related to increased incidence of hemorrhagic stroke.[19] Low albumin, globulin ratio was found to predispose to recurrent strokes.[20]
Serum lipids have been linked to a higher risk of ischemic stroke. [21] An inverse association exists for total cholesterol and cerebral hemorrhage. A greater mortality is observed from hemorrhagic stroke with serum cholesterol levels under 160 mg/dL.[22] In a recent study total cholesterol measured within 24 hours suggested that higher levels of cholesterol were associated with a favorable early outcome after ischemic stroke.[23] We could not establish any prognostic significance of cholesterol levels.
In conclusion, a high ESR, total leukocyte count, creatinine and SGPT and a low GCS score at admission are independent predictors of 30-day fatality in acute stroke.
References
| 1. | Woo E, Chan YW, Yu YL, Huang CY. Admission glucose level in relation to mortality and morbidity outcome in 252 stroke patients. Stroke 1988;19:185-191. Back to cited text no. 1 |
| 2. | Kochanek PM, Hallenbeck JM. Polymorphonuclear leucocytes and monocytes/macrophages in the pathogenesis of cerebral ischemia and stroke. Stroke 1992;23:1367-79. Back to cited text no. 2 [PUBMED] |
| 3. | Chamorro A, Vila N, Ascaso C, et al. Early prediction of stroke severity. Role of erythrocyte sedimentation rate. Stroke 1995;26:573-6. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Czlonkowska A, Ryglewicz D, Lechowicz W. Basic analytical parameters as the predictive factors for 30 day case fatality rate in stroke. Acta Neurol Scand 1997;95:121-4. Back to cited text no. 4 [PUBMED] |
| 5. | Hatano S. Experience from multicentric stroke register-a preliminary report. Bull World Health Organ 1976;54:541-553. Back to cited text no. 5 |
| 6. | Demchuk AM, Buchan AM. Predictors of stroke outcome. Neurology Clin 2000;19:455-72. Back to cited text no. 6 |
| 7. | Chambers BR, Norris JW, Shurvell BL et al. Prognosis of acute stroke. Neurology 1987;37:221-5. Back to cited text no. 7 [PUBMED] |
| 8. | D'Erasmo E, Aliberti G, Celi FS, et al. Platelet count, mean platelet volume and their relation to prognosis in cerebral infarction. J Intern Med 1990;227:11-4. Back to cited text no. 8 |
| 9. | Wilhelmsen L, Svardsudd K, Korsan-Bengtsen K, et al. Fibrinogen as a risk factor for stroke and myocardial infarction. N Engl J Med 1984;311:501-5. Back to cited text no. 9 [PUBMED] |
| 10. | Helgason CM. Blood glucose and stroke. Stroke 1988;19:1049-53. Back to cited text no. 10 [PUBMED] |
| 11. | Nedergaard M. Transient focal ischemia in hyperglycemic rats is associated with increased cerebral infarction. Brain Res 1987;408:79-85. Back to cited text no. 11 [PUBMED] |
| 12. | Alex M, Baron EK, Goldenberg S, Blumenthal HT. An autopsy study of cerebrovascular accident in diabetes mellitus. Circulation 1962;25:663-73. Back to cited text no. 12 [PUBMED] |
| 13. | Mohr JP, Rubenstein LV, Tatemichi TK, et al. Blood sugar and acute stroke: The NINCDS Pilot Stroke Data Bank (abstrack). Stroke 1985;16:143. Back to cited text no. 13 |
| 14. | Melamed E. Reactive hyperglycemia in patients with acute stroke. J Neurol Sci 1976;29:267-75. Back to cited text no. 14 [PUBMED] |
| 15. | Candelise L, Landi G, Orazio EN, Boccardi E. Prognostic significance of hyperglycemia in acute stroke. Arch Neurol 1985;42:661-3. Back to cited text no. 15 [PUBMED] |
| 16. | Pulsinelli WA, Levy DE, Sigsbee B, et al. Increased damage after ischemic stroke in patients with hyperglycemia with or without established diabetes mellitus. Am J Med 1983;74:540-4. Back to cited text no. 16 [PUBMED] |
| 17. | Adams HP, Olinger C, Biller J et al. Usefulness of admission blood glucose in predicting outcome of acute cerebral infarction (abstract). Stroke 1987;18:296. Back to cited text no. 17 |
| 18. | Woo J, Lau E, Kay R, et al. A case control study of some hematological and biochemical variables in acute stroke and their prognostic value. Neuroepidemiology 1990;9:315-20. Back to cited text no. 18 [PUBMED] |
| 19. | Choi-Kwon S, Yang YH, Kim EK, et al. Nutritional status in acute stroke: Undernutrition versus overnutrition in different stroke subtypes. Acta Neurol Scand 1998;98:187-92. Back to cited text no. 19 [PUBMED] |
| 20. | Beamer N, Coull BM, Sexton G, et al. Fibrinogen and the albumin-globulin ratio in recurrent stroke. Stroke 1993;24:1133-9. Back to cited text no. 20 [PUBMED] |
| 21. | Sridharan R. Risk factors for ischemic stroke: A case control analysis. Neuroepidemiology 1992;11:24-30. Back to cited text no. 21 [PUBMED] |
| 22. | Lindenstrom E, Boysen G, Nyboe J. Influence of total cholesterol, high density lipoprotein cholesterol and triglycerides on risk of cerebrovascular disease: The Copenhagen City Heart Study. Br Med J 1994;309:11-5. Back to cited text no. 22 |
| 23. | Vauthey C, deFreitas GR, van, Melle G, et al. Better outcome after stroke with higher serum cholesterol levels. Neurology 2000;54:1944-9. Back to cited text no. 23 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04067t2.jpg]
[ni04067t1.jpg]
[ni04067t3.jpg]
|

{kind=link}
{kind=link}
{kind=link}