 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 224-227 Original Article Increased depressant effect of phenytoin sodium as compared to carbamazepine on cortical excitability: A transcranial magnetic evaluation Goyal V, Bhatia Manvir , Behari M Department of Neurology, All India Institute of Medical Sciences, New Delhi
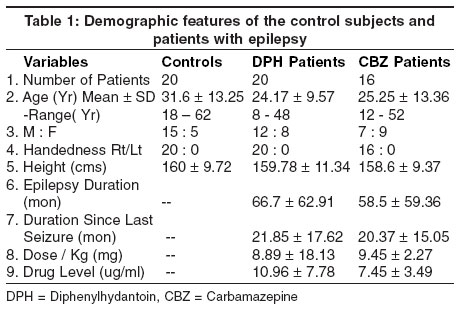
Correspondence Address:Prof. of Neurology, Dept. of Neurology, C. N. Centre, All India Institute of Medical Sciences, New Delhi - 110029 Code Number: ni04068 Abstract To evaluate the effect of monotherapy (phenytoin sodium (DPH) and carbamazepine (CBZ) on the threshold intensity (TI), cortical latency (CL), central conduction time (CCT), using transcranial magnetic stimulation (TMS). A single pulse transcranial magnetic stimulation was used for recording the motor-evoked potentials (MEP) from the thenar muscles of both hands, in 36 patients with well-controlled epilepsy on monotherapy, with normal EEG and imaging studies. The TI, CL, CCT and the MEP amplitude were recorded and compared with 20 healthy controls. The threshold intensity was significantly higher in patients on DPH, (P<0.05) with a significant decrease in the MEP amplitude when compared with controls (P<0.05). Anticonvulsants alter the excitability of human motor pathways in epileptic subjects. This effect differs among the drugs used; DPH had a greater depressant effect on the excitability than CBZ in the present study. Keywords: Cortical excitability, magnetic stimulation, epilepsy Introduction Transcranial magnetic stimulation (TMS) has been used to investigate a variety of clinical conditions with corticospinal pathway involvement. This is a pain-free, non-invasive and easy to use method without direct contact with the underlying skin.[1],[2] TMS has been uncommonly used in patients with epilepsy due to the hypothetical risk of inducing the seizures. However, a large number of studies in patients with epilepsy using TMS are available in the literature demonstrating the safety of this procedure.[3],[4],[5],[6],[7],[8] Previous studies in patients with epilepsy, mostly in chronic and refractory epilepsy, have shown that the predominant abnormality is a reversible decrease of the excitability of the central motor pathways due to antiepileptic drugs.[3],[9],[10] Chen et al studied the effect of orally administered phenytoin sodium in a total dose of 18mg/kg (in three equally divided doses over 6 hours) in healthy individuals on various TMS parameters.[11] They observed an increase in the motor threshold in all the subjects but there was no effect on motor-evoked potential amplitude, silent period duration and intracortical excitability during rest and voluntary muscle contraction. Ziemann U et al studied the effect of a single oral dose of different anticonvulsants on healthy individuals and reported a change in the intracortical excitability by GABA-controlled interneuronal circuit in the motor cortex.[12] In the above-mentioned studies, the effect of various anticonvulsant drugs administered as single doses in healthy volunteers has been evaluated. Materials and methods We studied patients with epilepsy attending the outpatient clinic of the Department of Neurology, All India Institute of Medical Sciences (AIIMS), New Delhi. All patients with epilepsy were on regular monotherapy (DPH or CBZ). They were seizure-free for a minimum of 3 months with normal electroencephalogram and normal imaging studies (contrast enhancing computerized tomography-CECT or magnetic resonance imaging-MRI). All the patients with uncontrolled seizures, progressive neurological disorders and systemic disorders were excluded. Patients with implant (cardiac pacemaker, intracranial aneurysm clips and metallic orthopedic implants) and pregnant women were also excluded. The controls were healthy subjects, non-relative friends of patients with epilepsy or attendants of the patients admitted to the neurology wards of the Department of Neurology of our hospital. The height and weight of all the subjects were recorded. Informed consent was taken from all the patients and healthy controls. Detailed history regarding birth, milestones, febrile convulsions in childhood, head injury, family history of epilepsy, focal neurological deficit in the past (in relation to epilepsy or otherwise) and mental retardation was noted. The duration of epilepsy, type of seizures (classified according to ILEA classification), period since last seizure, duration of present medication (DPH or CBZ) and frequency of seizures (in the last one year and prior to it) were recorded. Electrophysiological studies were done on both sides of the body in each subject. F-waves were recorded from the median nerve from the abductor pollis brevis (APB).[13] The active electrode was applied to the muscle belly of APB with the reference electrode placed 3 cm distally on the thumb. Twenty readings were recorded with supra-maximal stimulation of the median nerve at the wrist and the latency of the shortest f-wave response was recorded. The magnetic stimulation of the motor cortex and the cervical region was accomplished with a Magnetic stimulator- D190 circular magnetic coil (Digitimer Ltd, Hertfordshire, England) with coil diameter of 9 cm, maximum coil energy of 1200 joules and maximum induced field of 1.5tesla at the center of the coil. The filter setting used was 100Hz low filter and 10KHz high filter. The stimuli were delivered as single shocks at a frequency of one every 10-20 seconds. Post-stimulus analysis time was 50 msec. The sensitivity was 2mV. Stimuli were applied to the contralateral scalp with the center of the coil kept tangentially at the vertex in the mid-saggital plane dissecting the inter-aural line. The direction of the current was clockwise when the left cortex was stimulated and anti-clockwise to stimulate the right side of the cortex.[8],[14] Signals were recorded with a conventional EMG machine (Sapphire Premiere, Medelec). The recording electrodes were applied as mentioned for recording the F-wave. The subjects were seated on a comfortable chair, asked to relax and the procedure of the study was explained to relieve anxiety. Threshold intensity (TI) was recorded with a relaxed target muscle. TI was taken as the minimum stimulus intensity (measured as a percentage of the maximum output intensity of the stimulator) which was needed to evoke a response> 20uV in 3 out of 5 trials.[11] IFCN committee guidelines were used for recording the TMS parameters.[15] For TI, magnetic stimulation was given at 5% increment after every 5 stimuli till the desired TI was recorded. TI was determined separately for each hemisphere. If no response was recorded even at maximum coil output (100%) then the patient / control subjects were asked to contract APB and if still no response was recorded then TI was taken as 100% for statistical calculation.[3] For CL and MEP amplitude, the strength of magnetic stimulation was increased to 40% above TI with thumb abducted at 45 degrees. The shortest onset latency and the maximum amplitude from 5 responses were noted.[13] CCT was calculated by subtraction of the peripheral latency obtained by cervical stimulation (Cx). Cx was determined by stimulating efferent roots and nerves directly at the C7 vertebral level. CCT is time taken by electric stimuli to travel from the cortex to the spinal motor neuron. As magnetic stimulation of the cervical region stimulated not only spinal neurons but also motor roots and even proximal brachial plexus, we calculated CCT by both F-wave and direct method.[1],[15],[16] When CCT was calculated by the F-wave method (CCT1), F-wave was determined as described previously. Time required for the stimuli to travel to the spinal motor neuron synapses was taken as 1 msec. In calculating CCT by the direct method (CCT2), Cx was subtracted from CL.[18] Cx was determined as described above. CCT1 = CL-1/2(M+F+1) CCT2=CL-Cx (F=F-wave latency for median nerve, M= CMAP latency for median nerve) Results of TI, CL and CCT in healthy subjects and in patients with epilepsy on mono-therapy were expressed as means and standard deviation. One-way analysis of variance was done to see any significant difference (P value of <0.05), then multiple range test was done to evaluate the difference between the groups. Also inter-hemispheric differences in TI, CL and CCT were compared. Paired t-test was conducted to assess the difference between the TMS parameters on right and left hemispheric stimulation. To assess the association between the variables, Pearson′s correlation coefficient was performed. The p value of <= 0.05 for two tailed probability was considered significant. Results Thirty-six patients with epilepsy [17 with primary generalized and 19 (10 with right and 9 with left) with simple or complex partial with or without secondarily generalized epilepsy] and 20 healthy controls were evaluated. [Table - 1] shows the demographic features of the patients with epilepsy and the control subjects. The mean age of the control subjects was 31.6 ± 13.25 years (range 18-62 years) and of patients with epilepsy on DPH therapy was 24.17 ± 9.57 years (range 8-48 years) and on CBZ was 25.25 ± 13.36 years (range 12-52 years). The age among these groups was comparable (P=0.1265). All the control subjects and patients with epilepsy were right-handed. Other demographic features were comparable in all the groups. There was no significant difference in height, duration of epilepsy and duration since the last seizure in both groups. None of the subjects reported adverse side-effects. None had seizure during or within the 1-week follow-up period after TMS. The procedure was comfortable and acceptable. Discussion The present study evaluated 36 patients with epilepsy (20 on DPH and 16 on CBZ) and 20 healthy individuals. TMS was done to evaluate the effect of monotherapy (with DPH or CBZ) on TI, CCT, CL and MEP amplitude in all the patients. There was a statistically significant increase in TI and a decrease in MEP amplitude in patients on DPH (on right hemispheric stimulation). Acknowledgements We appreciate the technical help of our technical officers Mr. M. S. Bisht and Mr. R. Singh and the statistical assistance by Mr. Rajbeer. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04068t2.jpg] [ni04068t1.jpg] |
| |||||||||

{kind=link}
![[Table 2]](/showimage?ni/photo/ni04068t2.jpg){kind=link}