 |
search
for |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 228-232 Original Article p53 protein alterations in adult astrocytic tumors and oligodendrogliomas Nayak Anupma , Ralte Angela Mercy , Sharma Mehar Chand , Singh Varinder Paul , Mahapatra Ashok Kumar , Mehta Veer Singh , Sarkar Chitra Departments of Pathology, All India Institute of Medical Sciences, New Delhi
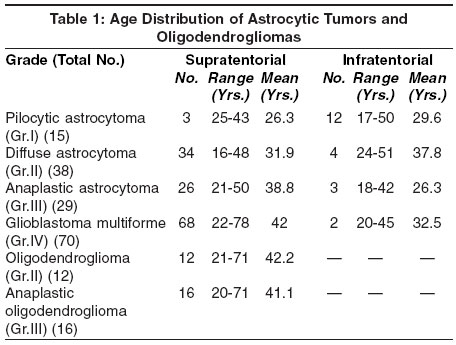
Correspondence Address:Professor, Room No. 1083, 1st Floor, Department of Pathology, All India Institute of Medical Sciences, Ansari Nagar, New Delhi - 110029 Code Number: ni04069 Abstract BACKGROUND: p53 is a tumor suppressor gene implicated in the genesis of a variety of malignancies including brain tumors. Overexpression of the p53 protein is often used as a surrogate indicator of alterations in the p53 gene. AIMS: In this study, data is presented on p53 protein expression in adult cases (>15 years of age) of astrocytic (n=152) and oligodendroglial (n=28) tumors of all grades. Of the astrocytic tumors, 86% were supratentorial in location while remaining 14% were located infratentorially - 8 in the the cerebellum and 13 in the brainstem. All the oligodendrogliomas were supratentorial. MATERIALS AND METHODS: p53 protein expression was evaluated on formalin-fixed paraffin-embedded sections using streptavidin biotin immunoperoxidase technique after high temperature antigen retrieval. RESULTS: Overall 52% of supratentorial astrocytic tumors showed p53 immunopositivity with no correlation to the histological grade. Thus, 58.8% of diffuse astrocytomas (WHO Grade II), 53.8% of anaplastic astrocytomas (WHO Grade III) and 50% of glioblastomas (WHO Grade IV) were p53 protein positive. In contrast, all the infratentorial tumors were p53 negative except for one brainstem glioblastoma. Similarly, pilocytic astrocytomas were uniformly p53 negative irrespective of the location. Among oligodendroglial tumors, the overall frequency of p53 immunopositivity was lower (only 28%), though a trend of positive correlation with the tumor grade was noted - 25% in Grade II and 31.5% in grade III (anaplastic oligodendroglioma). Interestingly, p53 labeling index (p53 LI) did not correlate with the histopathological grade in both astrocytic and oligodendroglial tumors. CONCLUSIONS: Thus, this study gives an insight into the genetic and hence biological heterogeneity of gliomas, not only between astrocytic tumors vs. oligodendrogliomas but also within astrocytic tumors with regard to their grade and location. With p53 gene therapy trials in progress, this will possibly have future therapeutic implications. Keywords: p53, immunohistochemistry, astrocytoma, oligodendroglioma Introduction The p53 gene, often referred to as the "guardian of the genome" is a tumor suppressor gene located on the short arm of Chromosome 17 at band 13.1 and consists of 11 exons.[1],[2],[3] It acts as a "molecular policeman" in preventing the propagation of genetically damaged cells; either directly, by its participation in mechanisms of DNA repair, or indirectly by its induction of cell cycle arrest and/or apoptosis in damaged cells. Further, recent data indicate its role in angiogenesis and tumor invasion. In keeping with its critical "gatekeeper" function, mutations of this gene are now implicated in the genesis of a variety of malignancies.[1],[2],[3] The normal p53 gene encodes a p53 kDa nuclear phosphoprotein ("wild type" p53 protein) which has a very short half life and is present in such small amounts within the normal cell nucleus that it cannot be detected by routine immunohistochemical methods.[3],[4],[5],[6] Mutations of the p53 gene result in the alteration of its protein and this "mutant" protein being metabolically more stable with a longer half life than the "wild protein", accumulates in the nucleus reaching a threshold of immunohistochemical detection. Based on these differences between the "wild" and "mutant" p53 proteins, immunohistochemistry has been extensively used to screen tumors for the presence of detectable p53 protein, thus indirectly indicating the presence of p53 gene alterations.[3],[4],[5],[6] There is growing evidence of the role of p53 gene alterations in the initiation, recurrence and progression of astrocytic tumors of Grades II, III and IV.[3],[4],[5],[6],[7],[8],[9],[10],[11],[12],[13],[14],[15],[16],[17],[18],[19],[20] However, its role in pilocytic astrocytomas (WHO Grade I) remains controversial.[21],[22],[23] Recent evidence also indicates that there may be different genetic alterations in pediatric and adult astrocytic tumorigenesis.[24],[25],[26],[27],[28],[29],[30] In contrast, oligodendrogliomas have been studied only sporadically for p53 protein expression, with the reported incidence varying from 30% to 75%.[31],[32],[33],[34],[35],[36] Hence, this study was undertaken to evaluate p53 protein expression in adult astrocytic tumors and oligodendrogliomas of all grades. The objective was to establish any differences/nexus in p53 protein expression and hence in p53 gene alterations over this wide histopathological spectrum and thus gain an insight into the biological relationship between these tumors. Materials and Methods
The haematoxylin and eosin (H&E) stained slides of all 180 cases were reviewed by two pathologists (CS & MCS). Diagnosis and grading were confirmed in all cases using WHO criteria[12] after concomitant agreement.
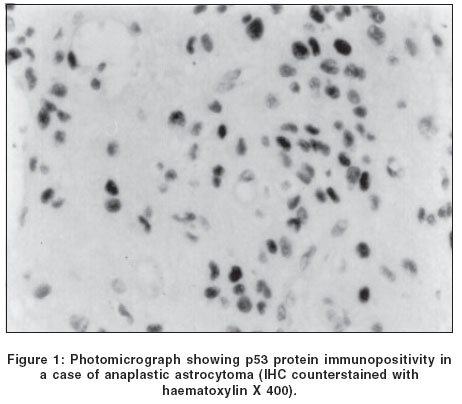
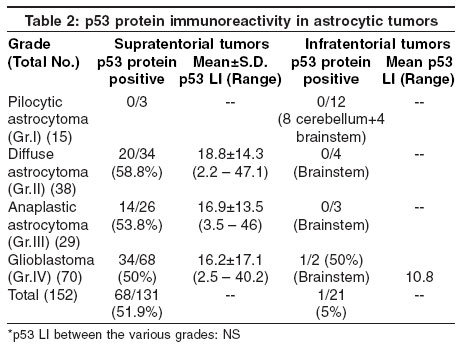
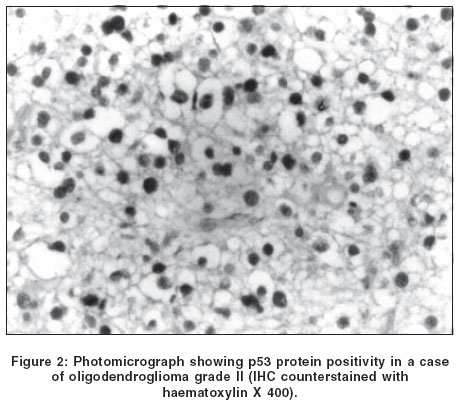
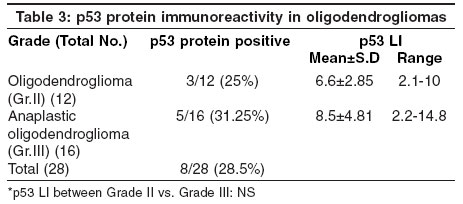
Firstly, high temperature antigen retrieval using microwave was done by immersing the sections in 10mM citrate buffer (pH 6.0) and heating inside a 600-watt microwave oven in full power for 30 minutes. The slides were then allowed to cool to room temperature and subsequently washed briefly with 0.05M Tris -hydrochloric acid (Tris-HCl) buffer, pH 7.4. During each batch of staining, appropriate positive and negative controls were used. Negative controls were achieved by omitting the primary antibody. Sections from a case of glioblastoma multiforme overexpressing the p53 protein were used as positive control. All incubations were done inside the humid chamber. Between each step, sections were washed in Tris-HCl buffer for 3X5 mts. The complete absence of nuclear stain or very occasional positively stained cells were regarded as negative. For p53 immunopositive cases, 1000 to 5000 tumor cells were counted in each case from at least 5 representative microscopical fields at high power magnification (400 X). An eyepiece pinhole was used to facilitate counting. In cases where an uneven distribution of immunolabeling was evident, fields from areas of maximal labeling were chosen for counting. Otherwise fields were chosen at random, taking care to avoid areas of necrosis (in cases of glioblastoma) as well as infiltrative edges of the tumor wherein tumor cells surrounded normal neurons and glia. The counting was done by two pathologists without knowledge of the histological grade. The results were calculated as a percentage of labeled nuclei. Results The grading of the 152 astrocytic tumors according to WHO criteria[12] was as follows: The majority of the astrocytic tumors (131/152 or 86%) were supratentorial in location. Only 21 tumors were infratentorial - 8 in the cerebellum and 13 in the brainstem. It is to be noted here that all the 8 cerebellar tumors and 4 of the brainstem tumors were pilocytic astrocytomas. All the 28 oligodendroglial tumors were supratentorial in location. The age and sex distribution of the astrocytic and oligodendroglial tumors is shown in [Table - 1]. p53 protein immunoreactivity was distinctly and uniformly absent in all pilocytic astrocytomas both in supra- and infratentorial locations. However, a distinct difference was noted between supratentorial diffuse astrocytomas, anaplastic astrocytomas and GBMs vs. their infratentorial counterparts. Thus, amongst 131 such supratentorial tumors, p53 immunopositivity was noted in 68 (51%) and distributed over all grades - 58.8% of diffuse astrocytomas, 53.8% of anaplastic astrocytomas and 50% of GBMs [Figure - 1]. There was no correlation between the frequency of p53 immunopositivity with the tumor grade and thus approximately 50% of the tumors in all grades were immunopositive [Table - 2]. In contrast, out of a total of 21 infratentorial astrocytic tumors, only 1 GBM (5%) showed p53 positivity. None of the diffuse and anaplastic brainstem astrocytic tumors were p53 immunoreactive. Similarly, all cerebellar and brainstem pilocytic astrocytomas were also p53 negative [Table - 2]. Among the oligodendrogliomas, only 8/28 (28.5%) cases demonstrated positivity for p53 protein [Figure - 2]. However, on comparing the grades, p53 protein positivity was slightly higher in anaplastic oligodendrogliomas (5/16 or 31.25%) as compared to Grade II tumors (3/12 or 25%) [Table - 3]. There was no significant difference in p53 LI between the various grades of astrocytic tumors or oligodendrogliomas [Table - 2] & [Table - 3]. Discussion Overexpression of the p53 protein is often used as a surrogate indicator of alterations in the p53 gene status, although it is now well documented that p53 protein overexpression may occur for reasons other than mutation in the p53 gene.[4],[5],[6],[11] The present study revealed differences in p53 protein expression between astrocytic tumors and oligodendrogliomas. Further, heterogeneity in p53 protein immunoreactivity amongst astrocytic tumors was observed with regard to their histological grading and location. This is the first Indian study from a single center documenting such heterogeneity. Thus, approximately 50% of supratentorial diffuse astrocytomas, anaplastic astrocytomas and GBM showed p53 protein immunoreactivity. Similar observations have also been reported in earlier studies[3],[4],[5],[6] which have detected p53 protein immunohistochemically in approximately 15-40% of diffuse astrocytomas, 35-60% of anaplastic astrocytomas and 35-70% of GBMs. Further confirmation has been made available from genetic studies which have revealed allelic loss of chromosome 17p and p53 mutations in approximately one-third of all three grades of adult astrocytic tumors. All this indicates that the inactivation of the p53 tumor suppressor gene is an important early genetic event in tumorigenesis of adult supratentorial astrocytic tumors.[7],[8],[9],[10],[12] In contrast, infratentorial (brainstem) astrocytic tumors were found to be rarely p53 protein positive in this study (5%). It is now well established that GBMs develop by either one of the two pathways - one that requires p53 inactivation (secondary GBM) and the one that requires epidermal growth factor receptor (EGFR) amplification (primary or de novo GBM).[12],[37] Thus, p53 mutation and p53 protein accumulations have been noted in 10% and 35% of primary GBMs respectively, while in secondary GBMs the incidence has been >65% and >90% respectively.[37],[38],[39],[40],[41] Brainstem GBMs in adults are rare and possibly most are primary/de novo,[37] while in the supratentorial location a considerable percentage of adult GBMs are secondary. This may account for the differences in p53 protein expression between supratentorial astrocytic tumors of grades II to IV versus their brainstem counterparts. Studies on EGFR expression however need to be done to confirm this. Another interesting observation in this study was that pilocytic (grade I) astrocytomas were all uniformly p53 protein negative irrespective of their location. Earlier reports[21],[22],[23] have also shown that p53 mutations are either absent or rare in pilocytic astrocytomas, indicating that inactivation of the p53 possibly does not play a role in their evolution.[23] No distinct pattern of loss of any particular tumor suppressor gene has been reported in these tumors till date,[21] though the role of neurofibromatosis type 1 (NF 1) gene has been extensively studied. Thus, based on available evidence, pilocytic astrocytomas appear to be genetically different from other grades of astrocytic tumors and need further molecular investigations. Based on these differences observed in p53 protein expression, it may be suggested that p53 immunostaining can have potential diagnostic utility. Especially in small biopsies/stereotactic biopsies wherein there may be problems in deciding between pilocytic vs. diffuse astrocytoma, p53 immunopositivity if present will tilt the diagnosis in favor of the latter. However, negativity for p53 protein in such a situation will not be conclusive. This study also revealed that p53 protein expression was much lower in oligodendrogliomas (28.5%) as compared to that seen in supratentorial astrocytic tumors (52%). This is in keeping with genetic studies which have demonstrated p53 gene mutations only in 10-15% of these tumors,[31],[42],[43],[44] though immunoreactivity for p53 protein has been reported in a much higher percentage of cases.[32],[33],[34],[35],[45] In astrocytic tumors, no obvious relationship could be demonstrated between the frequency of p53 immunopositivity and the tumor grade which is similar to the results of previous studies.[3],[4],[5],[6] In contrast, p53 positivity increased with the histological grade in oligodendrogliomas. Barbireschi et al[33] reported p53 protein expression only in high grade oligodendrogliomas (3/11). Pavelick et al,[35] in a study of 56 cases noted 100% p53 positivity in malignant oligodendrogliomas whereas only 64% of Type II and 28% of Type I low-grade oligodendrogliomas showed positivity for p53, thus suggesting its correlation with tumor malignancy. Pal et al[45] noted p53 protein overexpression in 58.3% of high-grade oligodendrogliomas in contrast to only 8.3% of low-grade ones. Thus, similar to our study their overall frequency of p53 immunoreactivity in oligodendrogliomas was 34.5%. In contrast, Kros et al[32] in a large study of 84 oligodendrogliomas noted p53 immunoreactivity in 75% of their cases irrespective of grade. With regard to p53 LI, our results are in agreement with the reports of Saito et al,[36] and Kros et al[32] who observed that the mean p53 staining indices were not statistically significantly different between low and high-grade oligodendrogliomas. However, Hagel et al[34] proposed a cut-off p53 LI value of 2% which correlated well with the tumor grade and could be used as an independent predictor of survival. Thus, the present study revealed dissimilarities in p53 protein expression between astrocytic tumors with respect to their grade and location. Thus, p53 does not seem to play a major role in pilocytic astrocytomas unlike astrocytic tumors of Grades II to IV. More cases need to be studied to establish its role in adult brainstem gliomas as well as in the determination of the clinical outcome.[46] The present study also revealed differences between astrocytic tumors and oligodendrogliomas, thus reflecting basic differences in the biology of their initiation and progression. p53 alterations do not seem to be an early genetic event in most oligodendrogliomas unlike in adult supratentorial astrocytic tumors of Grades II to IV. Studies to look at other genetic pathways in oligodendrogliomas are therefore required. Acknowledgements The authors are grateful to the Indian Council of Medical Research (ICMR) for funding the grant. The technical help received from Mrs. Kiran Rani, Mr. Rajeshwar Khadia, Mr. Anil and Mr. Gajender is gratefully acknowledged. We also thank Mr. Kamal for secretarial assistance and typing of the manuscript. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04069t1.jpg] [ni04069f2.jpg] [ni04069t2.jpg] [ni04069f1.jpg] [ni04069t3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}