 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 233-237 Original Article Challenging epilepsy with antiepileptic pharmacotherapy in a tertiary teaching hospital in Sri Lanka Kariyawasam SH, Bandara Namal , Koralagama A, Senanayake Sunethra Dept. of Pharmacology, Faculty of Medicine, University
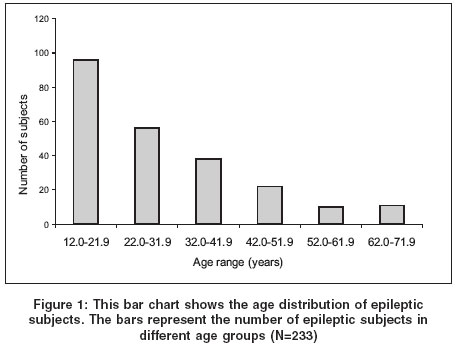
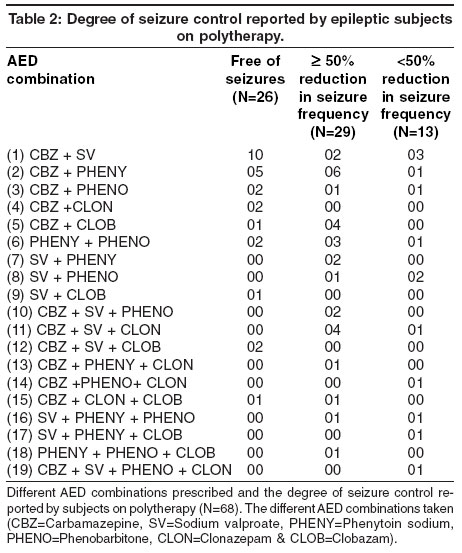
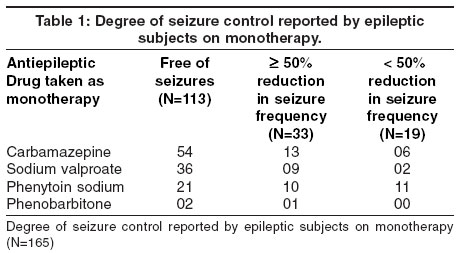
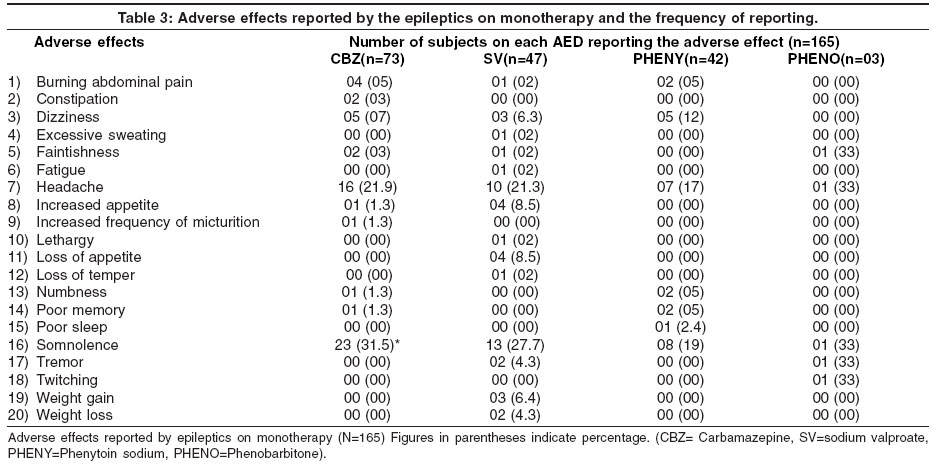
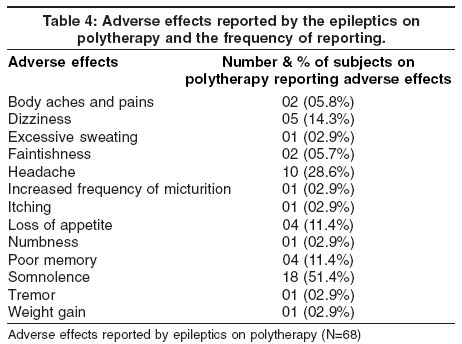
of Colombo Code Number: ni04070 Abstract The goal of antiepileptic drug (AED) therapy is to achieve a seizure-free state and eliminate the medical and psychosocial risks of recurrent seizures. Burden of epilepsy on the economy of a country may be largely due to the expenditure on AEDs. The adverse effects may influence the compliance to AEDs and effective control of epilepsy. We determined the pattern of AED use, the degree of epileptic control achieved and the adverse effects experienced by the epileptics in a Tertiary Teaching Hospital in Sri Lanka. Carbamazepine was found to be the most frequently used AED. Monotherapy was used on 70.8% of subjects. 86.27% of the study sample had achieved effective control of epilepsy with a 50% or more reduction in seizure frequency. Of them 72.64% were on monotherapy and they were either on carbamazepine, sodium valproate, phenytoin sodium or phenobarbitone. None of the new AEDs were prescribed to these patients. 50.9% on monotherapy and 51.5% on polytherapy reported adverse effects. Somnolence followed by headache was found to be the most frequently reported adverse effects by those on monotherapy and polytherapy both. This study shows that most epileptics can be effectively managed with the conventional AEDs with clinical monitoring. Introduction Epilepsy is a common neurological condition affecting 0.5-1% of population. The characteristic event in epilepsy is the seizure that may be detected by electroencephalography (EEG). Epidemiological studies of epilepsy from around the world have shown prevalence rates ranging from 0.9-57 per 1000 population, with higher prevalence rates for developing countries. Epilepsy causes a heavy burden on patients, their families and economy in both developed and developing countries.[1] The fundamental principles of managing epilepsy include making an accurate diagnosis and characterization of seizure type, choosing the most effective antiepileptic drug (AED) for the seizure type, pushing the dose to effect and exhausting monotherapy before using polytherapy or nonmedical therapies. The ultimate goal of antiepileptic therapy should be to achieve a seizure free state. However in some clinical trials a 50% or more reduction in seizure frequency is considered as a surrogate measure in determining the efficacy of AEDs. Burden of epilepsy on the economy of a country may be largely due to the expenditure on AEDs. Therefore it is important to consider the cost of drugs in achieving epileptic control, while giving the patients the best possible quality of life. Patient′s compliance to AEDs is a vital factor in achieving effective control of epilepsy. Since there are important, known adverse effects of AEDs, especially reported with long-term use, the patients′compliance to AEDs may be influenced by them. Therefore we thought it was important to determine the pattern of AED use in a tertiary hospital in Sri Lanka, the degree of epileptic control achieved and the adverse effects commonly experienced by our patients in order to make useful suggestions on management of epileptics to improve their quality of life. The objectives of this study were to determine: the frequency of using different AEDs in the outpatients′clinics managing epileptics at the North Colombo Teaching Tertiary Hospital (NCTH) in Sri Lanka, the degree of seizure control achieved by the patients with the treatment given from the clinics and the common adverse effects of AEDs experienced by the patients. Material and Methods This was a cross sectional descriptive study. The study population was selected from the epileptic patients attending adult medical and neurology clinics of the NCTH during one calendar month (01st - 31st October 2000). In Sri Lanka, patients above 12 years of age attended the adult clinics in the government hospitals of the Ministry of Health. Therefore the study sample included patients above 12 years of age. The criteria for including a subject in the study were that he/she has been diagnosed to have epilepsy by a Consultant Neurologist or a Physician with a clinical history, examination and relevant investigations including an EEG, has been on AED/s for more than eight weeks, not on any other medication and consented to take part in this study. There were two Neurology and three Medical clinics run at the NCTH for out patients over 12 years of age, that cared for epileptic subjects. Two Consultant Neurologists and three Consultant Physicians were responsible for giving care to patients attending these clinics. A questionnaire was designed according to the objectives. It composed of two sections: a patient administered section in Sinhala and an interviewer administered section in English. Further details were taken from patients′clinical records. A pilot study was carried out on the 19th of September 2000 in an adult Neurology clinic of the NCTH, with the first ten epileptic patients who satisfied the criteria described above to be included in the study. The pilot study ensured the clarity of the questionnaire. The data of this study was analyzed using the Statistical Package for Social Sciences (SPSS). Results The study group comprised of 233 subjects: 119 (51%) males and 114 (49%) females. The mean age of the subjects was 29.2 years: range 12-70 years. The majority of the subjects (41.2%) were in the 12-21.9 years age range. The Age distribution of the subjects is shown in [Figure - 1]. 165 subjects (70.8%) were on monotherapy and 68 (29.2%) were on polytherapy. [Figure - 2] shows the frequency of using different AEDs, showing separately their use as monotherapy and in polytherapy regimes. Carbamazapine was found to be the most frequently used AED, being used on 39% of the subjects as monotherapy or in combination. There were 19 different AED combinations used in this group of epileptics [Table - 2] and the most frequently used AED combination was carbamazepine + sodium valproate. [Table - 1] shows the number of subjects on different AEDs as monotherapy who reported different degrees of seizure control (free of seizures, ³ 50% reduction in seizure frequency and less than 50% reduction in seizure frequency). [Table - 2] shows the different AED combinations used on the 68 subjects on polytherapy and the number of subjects reporting different degrees of seizure control. 113 (68.5%) subjects on monotherapy and 26 (38.2%) subjects on polytherapy were free of seizures with the AEDs they were receiving from the clinics. 74.0% getting carbamazepine, 76.6% getting sodium valproate and 50% getting phenytoin sodium as monotherapy were free of seizures. Out of the 233 subjects a total of 139 (59.66%) were free of seizures and another 62 (26.61%) had a ³ 50% reduction in seizure frequency with the treatment received from clinics. 50.9% on monotherapy and 51.5% on polytherapy reported experiencing various adverse effects of the AEDs they were taking. [Table - 3] shows the adverse effects reported by the epileptics on monotherapy and the number and percentage of subjects on each AED reporting them. [Table - 4] shows the adverse effects reported by the subjects on polytherapy and the number and the percentage of subjects on polytherapy reporting them. Somnolence was the most frequently reported adverse effect by epileptics on monotherapy as well as on polytherapy. Of the epileptics who reported somnolence, with monotherapy 31.5% were on carbamazepine and 27.7% were on sodium valproate. Discussion The male: female ratio of the epileptics who sought treatment from the clinics was almost 1:1 (51% males and 49% females). The majority of the subjects (41.2%) were in the 12-21.9 years age group. Even though the diagnosed epilepsy syndrome is one major factor that determines the choice of AEDs, a definitive syndromic diagnosis has not been made on all the patients of our study sample and therefore we are unable to show the distribution of patients according to different epileptic syndromes. 70.8% of subjects were on monotherapy. In keeping with the recommended principles of antiepileptic therapy, the practice of polytherapy was relatively low (29.2%) in this Sri Lankan tertiary center. The most frequently prescribed AED in these clinics as monotherapy and in combinations was carbamazepine followed by sodium valproate. The most frequently prescribed AED combination was carbamazepine + sodium valproate. Phenobarbitone has been used as monotherapy only on 03 subjects in this study group and was used in polytherapy in 23 patients on eight different combinations. Even though phenobarbital is the oldest of the currently available AEDs, it has lost its popularity in this era. Phenobarbitone is seldom used after infancy in developed countries. Out of the epileptics on monotherapy 68.5% were free of seizures and another 20% have achieved 50% or more reduction in seizure frequency. Reynolds and Shorvon[2] have shown that 70-80% of patients can be efficiently controlled with monotherapy. The seizure free percentage out of the total number of subjects receiving carbamazepine (74.0%) and sodium valproate (76.6%) as monotherapy were almost equal. Phenytoin sodium was used on 37.2% of subjects as monotherapy and of them only 50% was free of seizures. These results show that Carbamazepine and Sodium valproate are more efficient in achieving epileptic control than Phenytoin sodium. Even though our center of study was a tertiary teaching hospital there were no facilities for measuring the plasma concentration of AEDs, and dosage was adjusted and determined on clinical grounds. A study done in Italy by Jannuzzi et al[3] has shown that there were no significant differences between the epileptics managed with monitoring of serum levels of AEDs and on clinical grounds alone, with regards to achieving epileptic control and frequency of adverse effects. Considering the percentage of epileptics who have achieved significant control of epilepsy in our study (see results), together with the results of Jannuzzi et al[3] we suggest that with the AEDs most commonly used, monitoring the serum levels of these drugs in selected patients and in special situations is likely to be more useful than routine measurements in large clinic populations. This suggestion is more relevant to developing countries where WHO[6] has reported to have epileptics not receiving treatment due to the cost involved. It is more important to make the AEDs available to more patients, than to have extensive facilities for therapeutic monitoring. In this group of patients only 38.2% of subjects on polytherapy were free of seizures in contrast to the 68.5% on monotherapy. This low percentage of seizure free subjects in the polytherapy group would have been due to most of them suffering from difficult to control epileptic syndromes. However 19 different AED combinations has been used on them. Therapeutic monitoring may be helpful in optimizing these AED combinations and doses. The percentage reporting adverse effects were only slightly higher in the subgroup on polytherapy (51.5%) than in the subgroup on monotherapy (50.9%). Somnolence followed by headache was found to be the most frequently reported adverse effects by the epileptics on monotherapy and polytherapy both. None of the new AEDs are available in the Sri Lankan government hospitals, but lamotrigine and topiramate are available in the private sector for patients to buy on prescriptions. Other new AEDs can be brought from overseas on a personnel license if prescribed by a medical consultant, but none of these patients have been prescribed new AEDs. 86.27% of the whole study group had achieved effective control of epilepsy with a 50% or greater reduction in seizure frequency. Of them 72.64% were those on monotherapy and they were either on carbamazepine, sodium valproate, phenytoin sodium or phenobarbitone. Clonazepam and clobazam were used in combination therapy. However recent statistics[1] from the private sector of Sri Lanka for a year (1st July 1999 - 30th June 2000) showed 1.67% of the expenditure by patients for AEDs being spent on lamotrigine.[4] A review by Perucca[5] states that when new AEDs are added to preexisting therapy in patients with refractory epilepsies, they improve seizure frequency in 15% to 40% of cases, but only rarely freedom from seizures is achieved. Perucca[5] also reports that new AEDs are not free of severe adverse effects and in newly diagnosed patients, the efficacy is similar to that of older agents. These facts on new AEDs considered together with our results raise the question whether the clinicians should promote the use of new AEDs in developing countries where one should be concerned about the cost of drugs, in order to reduce the burden on the patients and economy of a country, when effective control of epilepsy can be achieved with the less costly conventional AEDs. The new antiepileptic drugs may be a useful contribution in challenging epilepsy, but because of limited clinical experience and cost considerations their first line use cannot be recommended in most situations. The use of new AEDs should be reserved for use on epileptics not responding to conventional AEDs. A pharmacoepidemiologic and pharmacoeconomic study done in a tertiary referral center in South India has also shown carbamazepine to be the most frequently prescribed AED alone and in combination. The same study has shown an increase in the number of seizure free patients within the study sample with a decrease in the use of phenytoin sodium and an increase in the use of sodium valproate.[6] Results of this Indian study by Radhakrishnan et al[6] taken together with our results, strongly suggest making AEDs, carbamazapine and sodium valproate more available at a lesser cost by increasing their production locally in developing countries. Carbamazapine and sodium valproate given from NCTH to our study population were locally manufactured by the State Pharmaceutical Manufacturing Co-operation of Sri Lanka and imported from India. If steps are taken to cut down the costs involved in importing new AEDs and improve the local production of commonly used efficacious conventional AEDs, quality of life of many epileptics in developing countries may be improved. Acknowledgments We thank the two Consultant Neurologists and the three Consultant Physicians of the NCTH for their co-operation and the following fourth year medical students of the Faculty of Medicine, University of Kelaniya: Mr. H W Lasantha, Miss. W A S Loranganie, Mr. J J P Manjula, Miss. H A D Manoharee, Miss. D M S Manori, Miss. A S Marzooka, Mr. N W G Mahes, Mr. N S M Mendis and Mr. W J H Mendis for data collection.References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04070t4.jpg] [ni04070t3.jpg] [ni04070f1.jpg] [ni04070t1.jpg] [ni04070f4.jpg] [ni04070t2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}