 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 238-240 Case Report Role of magnetic resonance perfusion studies in moyamoya disease Khanna Paritosh C, Lath Chinar , Gadewar Swapna B, Patkar Deepak P Department of Magnetic Resonance Imaging, Nanavati Hospital, Mumbai
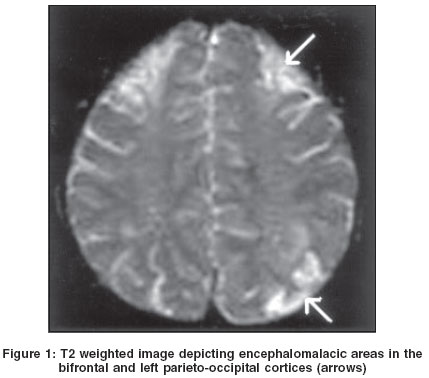
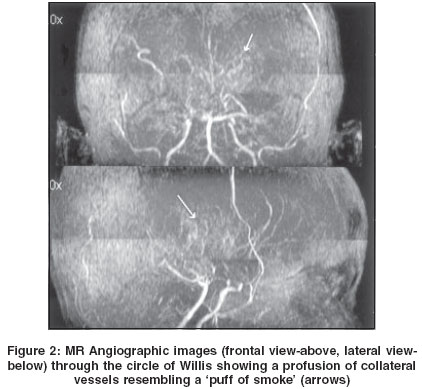
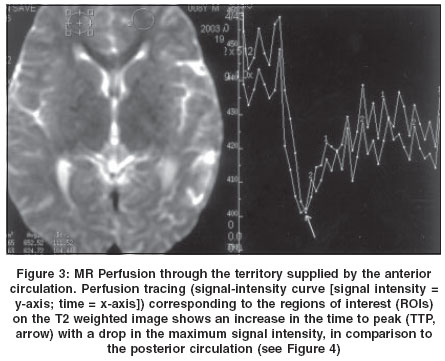
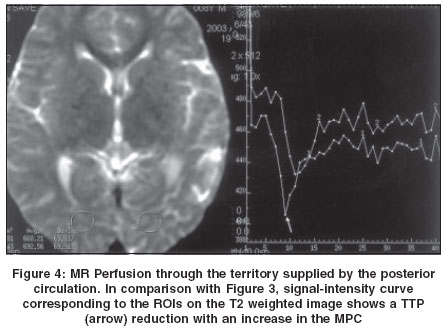
Correspondence Address:1211 B Everest Apartments, JPN Road, Seven Bungalows, Versova, Andheri (W), Mumbai - 400061 Code Number: ni04071 Abstract Moyamoya disease, Japanese for 'puff of smoke', is a rare disease that presents most commonly with recurrent TIAs (transient ischemic attacks) / stroke in childhood. Ischemic symptoms in patients with moyamoya disease are usually due to hemodynamically-mediated perfusion failure. Identification of abnormal tissue perfusion is an important aspect of the evaluation of these patients. We present the radiological features including the Magnetic Resonance (MR) Perfusion findings illustrating the hemodynamic changes of cerebral ischemia in a case of moyamoya disease.Keywords: Moyamoya disease, cerebral ischemia, magnetic resonance perfusion Introduction Moyamoya disease, a chronically progressive cerebrovascular occlusive disease affects the supraclinoid Internal Carotid Arteries (ICA) with prominent collateral formation, either of unknown etiology or secondary to neurofibromatosis and sickle cell anemia. Moyamoya affects the Japanese and Koreans and other ethnic groups.[1] MR Perfusion allows non-invasive investigation of tissue perfusion. Simultaneously acquired structural and diffusion images identify tissue with a normal diffusion but abnormal perfusion. In an acute stroke, such areas represent tissue-at-risk; in chronic cerebral ischemia, hypoperfused areas, not irreversibly damaged, are evident.[2] Conventional angiography, the ′gold-standard′ for depicting collaterals, nevertheless requires MRI to arrive at a diagnosis. This case demonstrates the utility of MRI and MR Perfusion as a stand-alone modality for moyamoya. Case Report An 8-year-old male presented with seizures and choreiform movements since 3½ years of age with slowing of mentation. Family history was negative. Examination revealed memory impairment, disorientation, hypotonia and chorea. Routine hematology, biochemistry and serology were negative. Computed Tomography revealed non-enhancing hypodense areas in the occipital and frontal regions bilaterally, suggesting infarcts. Basal ganglia collaterals were noted on post-contrast scans and moyamoya was considered as one of the differential diagnoses. Routine MRI, followed by Magnetic Resonance Angiography and MR Perfusion were obtained using a 1.5 Tesla System (Echospeed, GE Medical systems, Milwaukee, USA). MRI using T1 and T2 weighted (T1W, T2W) Spin Echo and FLAIR (Fluid-Attenuated Inversion Recovery) sequences, revealed well-defined wedge-shaped hyperintensities in bilateral frontal, parietal, parieto-occipital and left temporal cortices and subcortical white matter, suggestive of encephalomalacic areas [Figure - 1]. MR Angiographic images through the circle of Willis revealed near-complete occlusion of both supraclinoid ICAs. Both middle cerebral arteries (MCA) were not visualized. Both anterior cerebral arteries seemed to fill from the collaterals. Prominent vascular channels in the skull-base region (leptomeningeal collaterals) and basal ganglia resembled a ′puff of smoke′ [Figure - 2]. External carotid arteries (ECA) were prominent. Common carotid arteries and the basilar system were normal. MR Perfusion of the brain was obtained using dynamic T2FNx01W Gradient Echo EPI (Echo Planar Imaging, Time to Repeat [TR]: 1900ms; Time to Echo [TE]: 80ms) and delayed T1W Spin Echo sequences in multiple planes after administration of 8cc IV Gadolinium-DTPA. Comparison of the anterior and posterior circulations showed no significant variation in the amount of contrast uptake, suggesting good collateral formation. Delayed post-contrast T1W images confirmed this and depicted sluggish flow in the central skull-base and basal ganglia collaterals. The posterior circulation was more brisk than the anterior on the MR Perfusion, in that, the anterior circulation ′dip′ on the signal-intensity curve was less than the posterior circulation [Figure - 3] and [Figure - 4]. Perfusion through infarcts detected on routine MRI showed a flat curve indicating an ischemic core. At the periphery of these infarcts, a smaller ′dip′ represented an ischemic penumbra. Diffusion studies were essentially normal outside of the infarcted areas. Discussion Children present typically with recurrent episodes of sudden hemiplegia that might alternate sides. Fine involuntary movements of the extremities, seizures, slowly progressive mental impairment[3] and TIAs.[4] Children display a progressive course with ample collaterals while adults often have an arrested course with altered circulatory dynamics.[3] Imaging focuses on this collateral circulation, which forms owing to the occlusion of major proximal intracranial arteries. Typically, laboratory data are unremarkable. Screening EEG can be distinctive. 20 to 60 seconds following the termination of hyperventilation, high-voltage, slow waves return. The most consistent CT finding is a low-density area in the temporal white matter, a feature absent in our patient. However, angiography depicts the characteristic ′puff of smoke′, providing a definitive diagnosis. Also, Single Photon Emission Computed Tomography (SPECT) or Positron Emission Tomography (PET) are newer reference standards for assessing cerebral hemodynamics. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04071f4.jpg] [ni04071f2.jpg] [ni04071f1.jpg] [ni04071f3.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}