 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 241-242 Case Report Amyloidoma of the craniovertebral junction Shenoy SN, Raja A Department of Neurosurgery, Kasturba Medical College And Hospital, Manipal
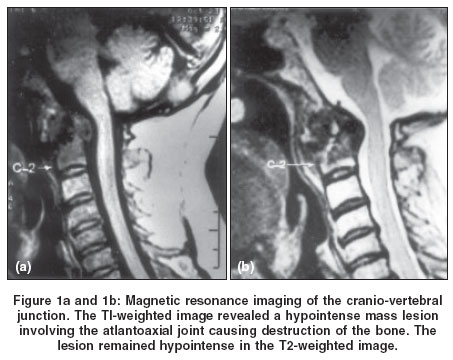
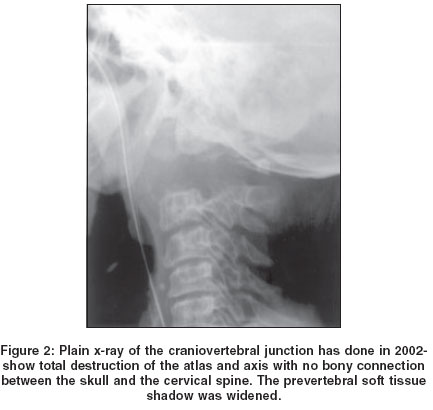
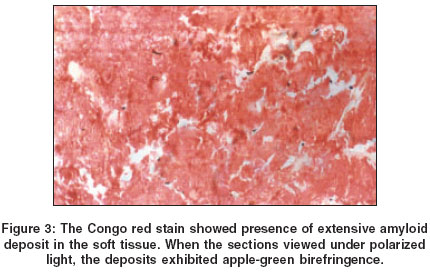
Correspondence Address:Department of Neurosurgery, Kasturba Medical College and Hospital, Manipal - 576119. Udupi Code Number: ni04072 Abstract We report a rare case of localized amyloidoma of the craniovertebral junction causing severe myelopathy and respiratory distress and death. The clinical features and the natural history of this rare condition are discussed. Keywords: Amyloidoma, craniovertebral junction, spine Introduction Primary solitary amyloidoma of bone is a rare disease characterized by the localized deposition of amyloid in which no plasma cell dyscrasias or abnormal serum proteins are detectable.[1],[2],[3],[4],[5],[6],[7] Till date only 20 cases of spinal amyloidoma have been reported in the literature. The involvement of the craniovertebral junction (CVJ) is rare.[8],[9],[10] We report an interesting case of localized amyloidoma of the CVJ who developed progressive destruction of the bone causing instability and death. Case Report A 58-year-old man presented with complaints of neck pain for three years and progressive weakness of the limbs and difficulty in swallowing for two months. Plain X-rays revealed destruction of the odontoid process. TI-weighted MR image revealed a hypointense mass lesion involving the atlantoaxial joint causing destruction of the bone. The lesion remained hypointense in the T2-weighted image [Figure - 1]a and [Figure - 1]b. When admitted, he was in a bed-ridden state. He was febrile. There was generalized wasting of the muscles. He had poor respiratory reserve with single breath count of 7. His throat examination revealed a smooth bulging of the posterior pharyngeal wall. His neck movements were painfully restricted. He was lying on the bed in a flexed posture. Motor system examination revealed spastic Grade 2-3/5 quadriparesis. He was placed on a Philadelphia collar. Investigations revealed destruction of the atlas and axis with no bony connection between the skull and the cervical spine. The prevertebral soft tissue shadow was markedly widened [Figure - 2]. Chest X-ray showed evidence of bilateral pneumonitis. The patient was placed on broad-spectrum antibiotics. Hematological investigations were normal except ESR=50mm/1hour. Liver function revealed hypoalbuminemia with normal bilirubin and enzymes. Bence-Zone protein was negative and serum electrophoresis showed no abnormality. Antinuclear antibodies and rheumatoid factors were negative. HIV and HbsAg were negative. As his respiratory function rapidly deteriorated due to worsening pneumonitis, he was intubated and given ventilatory support. He developed septicemia and hemodynamic instability. He was put on skull traction using Gardner-Wells traction. A blood stained fluid aspirated from the throat showed no evidence of acid-fast bacilli. He progressively worsened and developed bleeding diathesis and died. A transoral biopsy of the craniovertebral swelling was done immediately after the death. The Congo red stain showed presence of extensive amyloid deposits in the soft tissue [Figure - 3]. When the sections were viewed under polarized light, the deposits exhibited apple-green birefringence. Discussion Amyloidosis is a rare disorder, characterized by extracellular deposition of abnormal protein material that has characteristic fibrillar ultra structure and histological features.[11] Primary amyloidosis refers to the disorder in patients with no preceding or co-existing disease except multiple myeloma and secondary amyloidosis refers to the disorder in patients who also have inflammatory, infectious or neoplastic disease.[11] Amyloid deposits cause pathologic destruction by progressive intercellular accumulation and pressure atrophy of adjacent cells.[3] When deposited in the bone, the associated bony destruction mimics other aggressive pathologic processes, including infection and malignant disease. Amyloidosis of the spine is most frequently recognized in systemic amyloidosis, with or without co-existing multiple myeloma. However, localized spinal amyloidoma causing cord compression is very rare.[1],[5],[6] Localized amyloidosis may be entirely asymptomatic, or may cause symptoms through space-occupying effects.[5] The radiological features of spinal amyloidoma are not diagnostic or specific for amyloidoma and can simulate any destructive spinal lesions.[7] The amyloid lesions appear low signal in T1-weighted images and low to moderate signal on T2-weighted imaging.[5],[10] Although amyloidoma is rare, it should be included in the differential diagnosis of osteolytic lesions.[7] The various conditions considered in the radiological differential diagnosis include tuberculosis, metastatic tumors of the bone, plasma cell dyscrasias, chondrosarcoma, osteogenic sarcoma and metabolic diseases.[8] The diagnosis of localized amyloidoma requires an adequate tissue biopsy.[5] Congo red is the most widely used stain to differentiate amyloid from other hyaline deposits such as collagen.[11],[12] When the Congo red stained sections are examined under a polarizing microscope, a pattern of apple-green birefringence is usually visualized.[12] Once a diagnosis of amyloidoma is made, an attempt has to be made to detect any underlying chronic disorders including a complete bone survey.[8] References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04072f1.jpg] [ni04072f3.jpg] [ni04072f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}