
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 243-244
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 243-244
Case Report
Cauda equina paraganglioma presenting with intracranial hypertension: Case report and review of the literature
Sankhla Suresh , Khan GM
Department of Neurosurgery, Prince Aly Khan Hospital, Aga Hall, Nesbit Road, Mazagaon, Mumbai - 400 010
Correspondence Address:45/4, Chanchal-Smruti, G. D. Ambekar Road, Wadala, Mumbai - 400031
ssankhla@vsnl.com
Code Number: ni04073
Abstract An unusual case of intradural paragangliomas in the cauda equina region in a 29-year-old male is presented. The patient presented with signs and symptoms of raised intracranial pressure. The symptoms resolved after tumor resection.
Keywords: Paraganglioma, cauda equina, intracranial hypertension
Introduction Paragangliomas are benign and slow-growing neuroectodermal tumors commonly found in the adrenal medulla, carotid bodies, and glomus jugulare. Paragangliomas of the cauda equina are relatively rare.[1] Clinical manifestations produced by paragangliomas are non-specific and may include back pain and radicular symptoms. We report a case of paragangliomas which had unusual presenting symptoms. Case Report
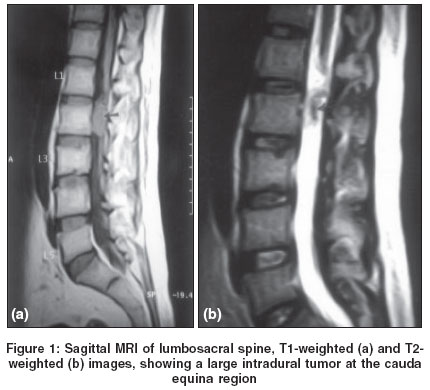
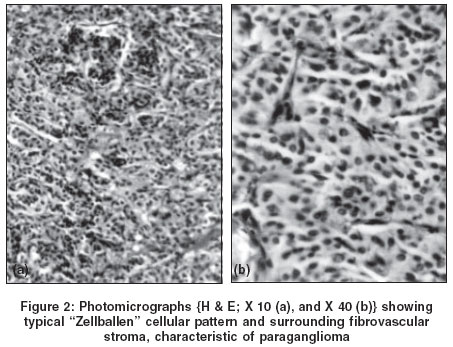
A 29-year-old man presented with a 9-month history of frontal headache associated with mild intermittent low backache. Neurological examination was normal except for bilateral papilledema. A gadolinium magnetic resonance imaging (MRI) of the brain was unremarkable. Cerebrospinal fluid (CSF) studies showed high opening pressure (>30 cm/H2O) and elevated protein level (>2,000 mg/dL). Spinal MRI demonstrated an intradural mass at L2 level, which was isointense with the cord on T1-, and hyperintense on T2-weighted images with a hypointense center [Figure - 1]a and [Figure - 1]b. A laminectomy was performed to remove a dark red, firm, vascular, and capsulated intradural tumor which was attached to the filum terminale and less firmly to the nerve roots and conus medullaris with fine arachnoidal strands. Histopathological study demonstrated a characteristic "Zellballen" pattern of the tumor cells associated with a delicate fibrovascular stroma, suggestive of a paraganglioma [Figure - 2]a and [Figure - 2]b). Further evaluation revealed no other spinal or adrenal tumor. His headache and back pain resolved completely at the follow-up four weeks later. Discussion Spinal paragangliomas are uncommon. Only a few cases have been reported since the first case of spinal paraganglioma was described. Miller and Torack[2] described the first case and since then only isolated cases have been reported in the literature. Generally, these tumors arise from the filum terminale and displace the nerve roots peripherally as they grow in size. Clinical symptoms produced by paragangliomas are non-specific and patients often present with features of the cauda equina syndrome including back pain, radicular symptoms, and bladder disturbances. Intracranial hypertension as a clinical manifestation of the spinal tumors is uncommon and has occasionally been observed with intradural tumors like ependymoma, schwannoma, astrocytoma, and meningioma.[3] Spinal paragangliomas presenting with the symptoms and signs of raised intracranial pressure are rare and have been reported in three cases.[4],[5],[6]
The pathogenesis of this rare clinical syndrome is uncertain. However, it has been postulated that the intracranial hypertension in these cases may be due to the elevated protein contents, which results in CSF absorption block by damaging Pacchionian granulations.[6] The CSF absorption defect may lead to the development of hydrocephalus, which may account for elevated intracranial pressure in some of these patients. The nature of the protein in the CSF has not been determined but it has been suggested that it is partly secreted by the tumors, or represents tumor breakdown products or fibrinogen. Subarachnoid hemorrhage is described in about 26% patients with spinal tumors and may be responsible for headache and papilledema by virtue of increased CSF proteins, CSF absorption defect and hydrocephalus.[3]
The secretion of a large amount of fluid by the tumors is also believed to be an etiological factor in the development of increased intracranial pressure.[3] However, hydrocephalus due to excessive CSF production has so far been documented only in patients with choroid plexus papilloma.[7] Blockage of the CSF outflow by arachnoid adhesions,[6] and tumors of the cervico-medullary junction,[3] as well as the intracranial leptomeningeal spread of distant spinal cord tumors,[8] have also been described to produce hydrocephalus and raised intracranial pressure.
Intracranial hypertension can occasionally develop as a result of obstruction in the CSF pathways due to fat droplets released intermittently by certain spinal lesions such as the epidermoid and dermoid cysts.[9]
However, in certain well-documented cases of spinal tumors, raised intracranial pressure has been recorded even with low CSF protein levels, normal ventricular size, and normal CSF absorption studies.[3] It therefore seems likely that in some of these cases the mechanism of intracranial hypertension is different and may be similar to that found in a number of inflammatory or immunologic disorders associated with benign intracranial hypertension.[10] Regardless of the mechanism of intracranial hypertension, the clinical symptoms and signs usually recover completely after the removal of the tumor as observed in our case. Acknowledgments The authors wish to express their grateful appreciation to Dr. R. F. Chinoy, Consultant Histopathologist, for her valuable help in providing the histopathological diagnosis and material for this article.
References
| 1. | Pigott TJ, Lowe JS, Morrell K, Kerslake RW. Paraganglioma of the cauda equina. Report of three cases. J Neurosurg 1990;73:455-8. Back to cited text no. 1 [PUBMED] |
| 2. | Miller CA, Torack RM. Secretory ependymoma of the filum terminale. Acta Neuropathol 1970;15:240-50. Back to cited text no. 2 [PUBMED] |
| 3. | Ridsdale L, Moseley I. Thoracolumbar intraspinal tumours presenting features of raised intracranial pressure. J Neurol Neurosurg Psychiatr 1978;41:737-45. Back to cited text no. 3 [PUBMED] |
| 4. | Hardten DR, Wen DY, Wirtschafter JD, Sung JH, Erickson DL. Papilledema and intraspinal lumbar paraganglioma. J Clin Neuro-Ophthalmol 1992;12:158-62. Back to cited text no. 4 [PUBMED] |
| 5. | Haslbeck KM, Eberhardt KE, Nissen U, Tomandl BF, Stefan H, Neundorfer B, et al. Intracranial hypertension as a clinical manifestation of cauda equina paraganglioma. Neurology 1999;52:1297-8. Back to cited text no. 5 [PUBMED] |
| 6. | Schijman E, Zuccaro G, Monges JA. Spinal tumors and hydrocephalus. Childs Brain 1981;8:401-5. Back to cited text no. 6 [PUBMED] |
| 7. | Milhorat TH, Hammock MK, Davis DA, Fenstermacher JD. Choroid plexus papilloma, proof of cerebrospinal fluid overproduction. Childs Brain 1976;2:273-89. Back to cited text no. 7 [PUBMED] |
| 8. | Maurice-Williams RS, Lucey JJ. Raised intracranial pressure due to spinal tumours: 3 rare cases with a probable common mechanism. Br J Surg 1975;62:92-5. Back to cited text no. 8 [PUBMED] |
| 9. | Cavazzani P, Ruelle A, Michelozzi G, Andrioli G. Spinal dermoid cysts originating intracranial fat drops causing obstructive hydrocephalus: Case reports. Surg Neurol 1995;43:466-9; discussion 469-70. Back to cited text no. 9 [PUBMED] [FULLTEXT] |
| 10. | Joynt RJ. Mechanism of production of papilledema in the Guillain-Barre syndrome. Neurology 1958;8:8-10. Back to cited text no. 10 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04073f2.jpg]
[ni04073f1.jpg]
|

{kind=link}
{kind=link}