
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 245-247
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 245-247
Case Report
Hashimoto's encephalopathy: Response to plasma exchange
Nagpal Tarun , Pande Sanjay
Department of Neurology Jabalpur Hospital & Research Centre and Netaji Subhash Chandra, Bose Medical College, Jabalpur
Correspondence Address:1769, Ratan Colony, Narmada Road, Jabalpur - 482001
tarunnagpal@hotmail.com
Code Number: ni04074
Abstract We report a case of 52-year-old female with steroid-unresponsive Hashimoto's encephalopathy. She underwent plasma exchange that resulted in marked clinical improvement.
Keywords: Hashimoto’s encephalopathy, myoclonus,
plasma exchange
Introduction Hashimoto′s encephalopathy is a rare disorder. It was first described by Brain et al in 1966.[1] Eighty-five cases have been reported in the literature so far.[2] The clinical picture is pleomorphic and cognitive impairment is a frequently reported symptom. There are two different clinical presentations. The vasculitic type is characterized by relapsing-remitting stroke-like episodes. The diffuse-progressive type shows insidious cognitive impairment, confusion, psychosis, somnolence and coma.[3] Usually, these patients respond to corticosteroids, however, various immunosuppressive treatments have been used in this condition, including azathioprine, cyclophosphamide, and intravenous immunoglobulin.[4] Plasmapheresis has been used where the response to corticosteroids has been incomplete.[5]
We report the case of a patient with slowly progressive cognitive impairment caused by Hashimoto′s encephalopathy, which showed minimal response to steroids but a rapid reversal of deteriorating neurological dysfunction was noted after the institution of plasma exchange. Case Report
A 52-year-old female presented with decline in memory and tremors of the extremities for last 6 months. On examination, there were mild extrapyramidal features in the form of mask-like facies and rest tremors of both the upper limbs with cogwheel rigidity. Her serum TSH was found raised (18.59 microIU/ml) with normal serum T3 (95 ng/dl), and serum T4 levels (4.8 microgm/dl). She received thyroid hormone replacement without any clinical response.
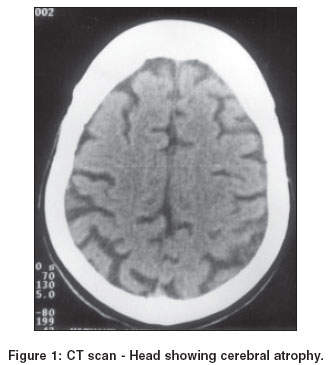
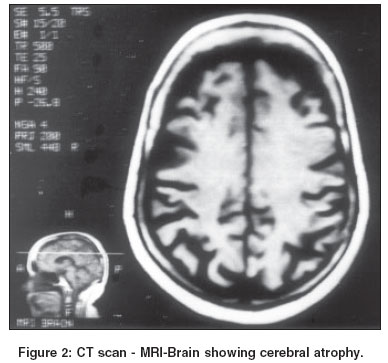
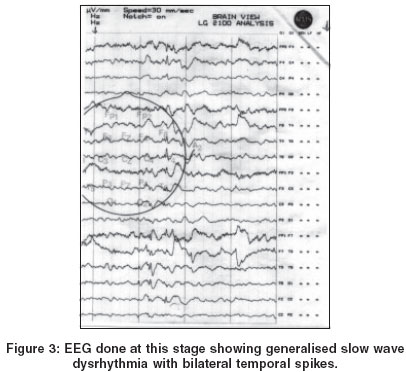
Her CT scan-Head [Figure - 1] and MRI-Brain [Figure - 2] showed cerebral atrophy. The CSF examination was within normal limits. EEG showed bihemispheric slowing without any epileptiform discharges. Over the subsequent 8 months, she developed difficulty in speaking with action myoclonus and a further decline in memory, cognition and visuospatial skills. Serum TSH continued to be high (25.9 microIU/ml), with normal serum T3 (101 ng/dl) and T4 (4.5 microgm/dl) levels. Her Serum Thyroid Peroxidase Antibody (thyroid microsomal antibody) level, done by ELISA technique was found 2860 U/ml (normal < 35 U/ml). Her serum thyroglobulin level was 0.24 ng/ml (normal<52 ng/ml). Her serum antinuclear antibody was negative. The patient was started on prednisolone 50 mg / day. The patient continued to deteriorate in cognition over the next 8 weeks. Her myoclonic jerks became frequent. She was unable to speak and had clouding of the sensorium. She further received 5 doses of 1 gm / day methylprednisolone and then prednisolone was resumed. The patient was followed up for a period of 3 months but there was no clinical improvement. Serum TSH levels were found normal (0.48 microIU/ml) and so was the free T4 level (1.86 ng/dl). However, the serum antithyroid peroxidase antibody level done by chemilumisence hormone assay was raised (1:202), normal range being less than 1:102. EEG done at this stage [Figure - 3] showed generalized slow wave dysrhythmia with bilateral temporal spikes. Plasmapheresis was instituted. Five cycles of 1800 ml of plasma was removed and replaced with albumin, plasma and hemaccel. Neurological improvement in the patient′s condition was noted after the third cycle of plasma exchange. Prednisolone 50 mg/day was continued. In a span of 10 days, the patient′s cognition improved markedly. Her bradykinesia and tremor has decreased and myoclonic jerks have disappeared. Fluency in speech has improved. She has resumed activities of daily living.Discussion Most patients of Hashimoto′s encephalopathy have normal MRI-Brain.[4],[6] However, abnormalities in brain MRI have been described.[7],[8] Cerebral atrophy is the most common non-specific neuroimaging finding as seen in our patient too. Cerebrospinal fluid is abnormal in more than 80% of the patients; with high protein levels and mononuclear pleocytosis.[3]
The EEG is helpful in evaluating and following patients with steroid-responsive encephalopathy associated with autoimmune thyroiditis in reflecting the degree of central nervous system (CNS) involvement, in determining whether their condition is better or worse, and in ruling out other causes of encephalopathy.[9] EEG findings include mild to severe generalized slowing, triphasic waves, epileptiform abnormalities, photomyogenic response, and photoparoxysmal response. Temporal spike discharges as seen in our patient have been well described in Hashimoto′s encephalopathy.[10]
The pathogenesis of Hashimoto′s encephalopathy remains unclear. Several theories have been proposed, including a generalized abnormality of the immune system, cerebral vasculitis, recurrent demyelination, or a toxic effect of thyrotropin-releasing hormone (TRH) on the CNS.[6],[7] An excessive, central release of TRH was held responsible for the epileptic seizures.[9] An abnormality of thyroid function itself cannot explain this condition, as many patients described in the literature are euthyroid either at the time of presentation or relapse. In our patient also, although the patient had subclinical thyroid abnormality initially, there was no clinical response to thyroid hormone replacement. The patient continued to worsen when the biochemical hormone levels were normal at a later stage.
An autoimmune basis is suggested by the high concentrations of antithyroid antibodies and improvement with immunosuppressive therapy. The precise role of antithyroid antibodies is also unclear: if they are to be implicated as pathogenic, then it is surprising that more cases of encephalopathy are not seen in patients with Hashimoto′s thyroiditis.
It is possible that the antithyroid antibodies in Hashimoto′s encephalopathy are a surrogate marker for other, as yet unknown, antibodies that cross the blood-brain barrier and initiate an autoimmune encephalopathy.[5]
By contrast with the Creutzfeldt-Jakob disease, which leads to death within a few months, patients with Hashimoto′s encephalitis often recover quickly when treated adequately. Corticosteroid therapy is the first choice. The successful administration of other immunosuppressants (methotrexate, azathioprine, cyclophosphamide) has been reported. Plasmapheresis should be used whenever the patient is unresponsive or poorly responsive to corticosteroid treatment. Epileptic seizures and myoclonus usually respond well to anticonvulsant drugs. Even with consistent therapy, relapsing disease courses are not rare, but the patients altogether clearly benefit from therapy.
References
| 1. | Brain L, Jellinek EH, Ball K. Hashimoto's disease and encephalopathy. Lancet 1966;2:512-4. Back to cited text no. 1 [PUBMED] |
| 2. | Chong JY, Rowland LP, Utiger RD. Hashimoto encephalopathy: Syndrome or myth? Arch Neurol 2003;60:164-71. Back to cited text no. 2 [PUBMED] [FULLTEXT] |
| 3. | Ares Luque A, Ballesteros Pomar MD, Hernandez EL. Hashimoto's encephalopathy, Neurologia 2002;17:628-32. Back to cited text no. 3 |
| 4. | Shaw PJ, Walls TJ, Newman PK, et al. Hashimoto's encephalopathy: A steroid-responsive disorder associated with high anti-thyroid antibody titres-report of 5 cases. Neurology 1991;41:228-33. Back to cited text no. 4 |
| 5. | Boers PM, Colebatch JG. Hashimoto's encephalopathy responding to plasmapheresis. J Neuro Neurosurg Psychiatr 2001;70:132. Back to cited text no. 5 |
| 6. | Peschen-Rosin R, Schabet M, Dichgans J. Manifestation of Hashimoto's encephalopathy years before onset of thyroid disease, Eur Neurol 1999;41:79-84. Back to cited text no. 6 |
| 7. | Kothbauer-Margreiter I, Sturzenegger M, Komor J. Encephalopathy associated with Hashimoto thyroiditis: diagnosis and treatment. J Neurol 1996;243:585-93. Back to cited text no. 7 |
| 8. | Bohnen NI, Parnell KJ, Harper CM. Reversible MRI findings in a patient with Hashimoto's encephalopathy. Neurology 1997;49:246-7. Back to cited text no. 8 |
| 9. | Latinville D, Bernardi O, Cougoule JP. Hashimoto's thyroiditis and myoclonic encephalopathy. Pathogenic hypothesis. Rev Neurol (Paris) 1985;141:55-8. Back to cited text no. 9 |
| 10. | Schauble B, Castillo PR, Boeve BF, Westmoreland BF. EEG findings in steroid-responsive encephalopathy associated with autoimmune thyroiditis. Clin Neurophysiol 2003;114:32-7. Back to cited text no. 10 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04074f1.jpg]
[ni04074f3.jpg]
[ni04074f2.jpg]
|

{kind=link}
{kind=link}
{kind=link}