
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 248-250
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 248-250
Case Report
Intracranial subfrontal schwannoma treated with surgery and 3D conformal radiotherapy
Prasad D, Jalali Rakesh , Shet T
Departments of Radiation Oncology, Tata Memorial Hospital, Parel, Mumbai - 400012
Correspondence Address:74, Department of Radiation Oncology, Tata Memorial Hospital, Parel, Mumbai - 400012
rjalali@medscape.com
Code Number: ni04075
Abstract
Subfrontal schwannoma not arising from the cranial nerves are rare tumors. A 19-year-old man presented with a large subfrontal extra-axial enhancing mass with a preoperative diagnosis of skull base meningioma. A subtotal resection of the tumor mass was carried out. Microscopic examination revealed it to be a schwannoma. The residual tumor was treated with fractionated three-dimensional conformal radiotherapy (3D CRT). The rationale of treating with radiotherapy in such cases is analyzed.
Keywords: Cerebral parenchyma, schwannoma, neurofibromatosis
Introduction Intracranial schwannomas arise usually from the vestibular part of the VIII cranial nerve and rarely from other cranial nerves, in descending order of frequency from the V, IX, VII, and III cranial nerves.[1] Schwannomas originating cranial nerves are usually associated with von Recklinghausen′s disease and can arise from any site within the cranium. Subfrontal schwannomas form a distinct subgroup and only 18 such cases have been reported.[1],[2],[3],[4],[5],[6],[7],[8] The treatment of choice in schwannomas is surgical excision, which is curative in a majority of patients.[1],[4],[9],[10] Radiotherapy is occasionally advocated for sub-totally excised tumors.[11],[12] However, since a majority of these patients have long-term survivals, they are particularly susceptible to developing late radiation sequel. Three-dimensional conformal radiotherapy (3D CRT) reduces the volume of normal brain irradiation as compared to conventional radiotherapy. Case Report
A 19-year-old man presented with a generalized tonic clonic convulsion. He also reported anosmia of two months duration. On examination, there were no cutaneous stigmata of neurofibromatosis. Neurological examination revealed bilateral mild sixth nerve weakness and anosmia. The rest of the neurological examination was unremarkable.
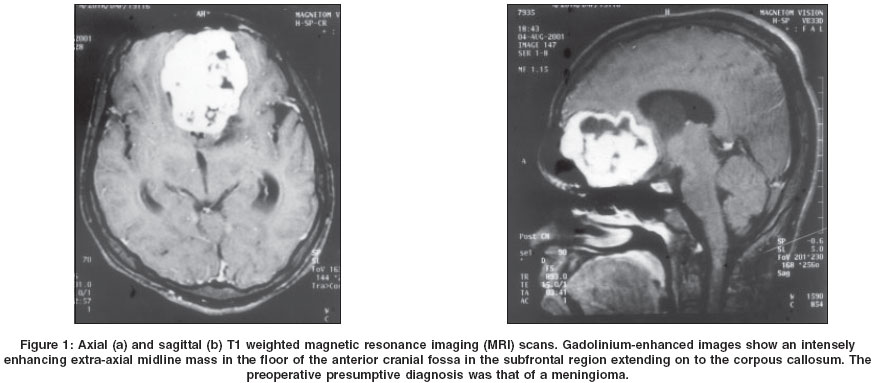
Computerized tomography (CT) scan and magnetic resonance imaging (MRI) of the brain revealed a fairly large heterogeneously enhancing mass lesion in the subfrontal region [Figure - 1]. The mass was predominantly hypointense on T1 weighted images, heterogeneously hyperintense on T2 weighted images and showed intense enhancement after injecting intravenous gadolinium. The mass was associated with minimal perilesional edema. In addition, there was a colloid cyst in the region of the foramen of Munro.
The surgical approach was by a bicoronal skin flap with frontoparietal craniotomy. Through a transcortical route, the lateral ventricle was entered into and with the assistance of an endoscope the colloid cyst was resected. Following the excision of the cyst wall, the brain became lax. The frontal lesion was then explored. The tumor was well identified, reddish, firm and moderately vascular. A radical excision of the tumor was done and the part of the tumor encasing the anterior cerebral artery branches was left behind. The patient tolerated the surgery well. While his anosmia improved subjectively, the sixth cranial nerve palsies persisted. A postoperative scan revealed a residual tumor, for which he was referred for radiotherapy. Histological examination revealed a typical schwannoma with cystic degeneration.
Because of his young age and the benign nature of the tumor, the patient was considered for high precision 3D CRT. The first step in the planning was immobilization of the patient in a customized thermoplastic shell, followed by a contrast enhanced CT scan in the treatment position. The CT scan slices taken with 5-mm thickness at 5-mm intervals were networked to the dedicated treatment planning computer workstation (Helax). Gross tumor volume (GTV), described as enhancing residual tumor, was contoured on each CT slice and a margin of 1 cm was grown in three dimensions to give the final planning target volume (PTV). Critical structures such as the eyes, optic nerves, optic chiasm, brainstem and pituitary hypothalamic axis were also contoured. Planning was done according to IRCU-50 criteria employing standard planning optimization including number of beams, beam weightage and wedges.[13] Treatment was delivered with three conformal fixed fields, conformation of each field being achieved by microleaf collimators (MLC) with a leaf separation of 1 cm at the isocenter. The dose was normalized to isocenter and the target volume irradiated to a dose of 54 Gy given in 30 daily fractions over a period of 6 weeks. The PTV was entirely covered by the 95% isodose line confirmed visually and on analysis of dose volume histograms generated by the planning computer. The patient tolerated radiotherapy well without any interruptions except expected side-effects like localized alopecia. Discussion As schwann cells are normally not present in the cerebral parenchyma, it is difficult to explain the origin of intracranial parenchymal schwannomas. Two main theories have been put forth to explain their pathogenesis. The developmental theory proposes that they arise from aberrant Schwann cells. Others suggest that they either originate from the multipotent mesenchymal cells or displaced neural crest cells, which form foci of Schwann cells termed as schwannosis within the CNS parenchyma.[3],[5],[14] The non-developmental theory proposes that the Schwann cells, which are present in the perivascular nerve plexuses and adrenergic nerve fibers innervating cerebral arterioles around large arteries in the subarachnoid space, develop into schwannoma.[15] Schwann cells are also seen in association with meningeal branches of the trigeminal and anterior ethmoidal nerves innervating the anterior cranial fossae and the olfactory groove.
Subfrontal schwannomas seem to form a distinct subgroup of intracranial schwannomas and only 18 cases have been reported in the literature so far. They are more common in males with a male to female ratio of 3:1 and an average age of 33 years (range 15 to 63). They tend to be seen slightly more commonly in the older age group with a mean age of 33 years as compared to other intracranial schwannomas.[4] Subfrontal schwannomas have been described to present as enhancing extra-axial masses on CT and MRI scans but in view of their extreme rarity, are almost never considered as first diagnosis. Our patient also had an accompanying colloid cyst located typically near the foramen of Munro. We located one case report where a subarachnoid cyst was identified along with a subfrontal schwannoma.[4] Both colloid and subarachnoid cysts are generally observed in young adults as are subfrontal schwannomas and therefore the association appears coincidental.
Surgery with a view to complete excision is the treatment of choice and can be often curative. Conventional radiotherapy in residual or recurrent schwannomas although employed rarely has been associated with good long-term tumor control.[11],[12] However, conventional radiotherapy may result in considerable treatment-related morbidity. Recently, there has been a lot of interest in high-precision techniques of radiation in brain tumors. Stereotactic radiosurgery (SRS) has been encouragingly used with promising efficacy as a suitable modality for the treatment of acoustic schwannomas, both as an alternative to surgery or in residual tumors.[16],[17] The advantage of stereotactic irradiation over conventional radiotherapy is its ability to conform the radiation doses to the target volume with a rapid fall-off of the dose to the surrounding normal brain and critical structures. SRS has been reported to achieve excellent local control rates of up to 97 % at 5 years with acceptable morbidity.[18] However, safe SRS is indicated only in small lesions, preferably less than 3 cm. Attempts have been also made to deliver stereotactic irradiation in a fractionated manner to minimize the toxicity but long-term data is still awaited.[10],[19],[20],[21]
3D CRT is an alternative high-precision technique of radiation, which has the ability to achieve beneficial dose differential between the tumor and adjacent normal tissues. The technique has demonstrated to result in a significantly reduced incidence of complications and also allows for dose escalation.[22] The advantages of these techniques are likely to be the greatest in young patients with benign and low-grade neoplasms associated with good long-term survival.
References
| 1. | Sarma S, Sekhar LN, Schessel DA. Nonvestibular schwannoma of the brain: A 7-year experience. Neurosurgery 2002;50:437-48. Back to cited text no. 1 [PUBMED] [FULLTEXT] |
| 2. | Boyd JH, Dalsaso TA Jr, Bee CS, Smith KR Jr, Martin DS. Subfrontal schwannoma with intracranial mucocele: A case report. Am J Otolaryngol 1997;18:72-5. Back to cited text no. 2 [PUBMED] |
| 3. | Frim DM, Ogilvy CS, Vonsattal JP, Chapman PH. Is intracerebral schwannoma a developmental tumor of children and young adults? Case report and review. Paediatr Neurosurg 1992;18:190-4. Back to cited text no. 3 [PUBMED] |
| 4. | Huang P, Zagzag D, Benjamin V. Intracranial schwannoma presenting as a subfrontal tumour: Case report. Neurosurgery 1997;40:194-7. Back to cited text no. 4 |
| 5. | Redekop G, Elisevich K, Gilbert J. Fourth ventricular schwannoma. Case report. J Neurosurg 1990;73:777-81. Back to cited text no. 5 [PUBMED] |
| 6. | Tan TC, Ho LC, Chiu HM, Leung SC Tan TC, Ho LC, et al. Subfrontal schwannoma masquerading as meningioma. Singapore Med J 2001;42:275-7. Back to cited text no. 6 |
| 7. | Tsai YD, Lui CC, Eng HL, Liang CL, Chen HJ. Intracranial subfrontal schwannoma. Acta Neurochir (Wien) 2001;143:313-4. Back to cited text no. 7 [PUBMED] [FULLTEXT] |
| 8. | Deogaonkar M, Goel A, Nagpal RD, Desai AP.Intraparenchymal schwannoma of the frontal lobe. J Postgrad Med 1994;40:218-9. Back to cited text no. 8 [PUBMED] [FULLTEXT] |
| 9. | Mazzoni A, Calabrese V, Moscinil. Residual and recurrent acoustic neuroma in hearing preservation procedures: Neuroradiologic and surgical findings. Skull base surgery 1996;6;105-12. Back to cited text no. 9 |
| 10. | Post KD, Eisenberg MB, Catalano PJ. Hearing preservation in vestibular schwannoma. J Neurosurg 1995;83;191-6. Back to cited text no. 10 |
| 11. | Maire JP, Caudry M, Darrouzet V, Guerin J, Trouette R, Bebear JP. Fractionated radiation therapy in the treatment of stage III and IV cerebello-pontine angle neurinomas: Long-term results in 24 cases. Int J Radiat Oncol Biol Phys 1995;32:1137-43. Back to cited text no. 11 [PUBMED] [FULLTEXT] |
| 12. | Wallner KE, Pitts LH, Davis RL, Sheline GE. Radiation therapy for the treatment of non-eight nerve intracranial neurilemmoma. Int J Radiat Oncol Biol Phys 1988;14:287-90. Back to cited text no. 12 [PUBMED] |
| 13. | CRU Report 50 Prescribing, recording and reporting photon beam therapy. International commission on radiation units and measurements 1993:1 Back to cited text no. 13 |
| 14. | Ramamurthy B, Anguli VC, Iyer CGS. A case of intramedullary neurinoma. J Neurosurg Psychiatry 1958;27:92-4. Back to cited text no. 14 |
| 15. | Nelson E, Rennes M. Inneravation of intracranial arteries. Brain 1970;93:475-90. Back to cited text no. 15 |
| 16. | Kondziolka D, Lunsford L, McLaughlin M, Flickinger JC. Long-term outcomes after radiosurgery for acoustic neuromas. NEJM 1998;339:1426-33. Back to cited text no. 16 |
| 17. | Pollock BE, Lunsford LD, Kondziolka D, Flickinger JC, Bissonette DJ, Kelsey SF, et al. Outcome analysis of acoustic neuroma management: A comparison of microsurgery and stereotactic radiosurgery. Neurosurgery 1995;36:215-24. Back to cited text no. 17 [PUBMED] [FULLTEXT] |
| 18. | lickinger JC, Kondziolka D, Niranjan A, Lunsford LD. Results of acoustic neuroma radiosurgery: An analysis of 5 years' experience using current methods. J Neurosurg 2001;94:1-6. Back to cited text no. 18 [PUBMED] |
| 19. | Fuss M, Debus J, Lohr F, Huber P, Rhein B, Engenhart-Cabillic R, Wannenmacher M. Conventionally fractionated stereotactic radiotherapy (FSRT) for acoustic neuromas. Int J Radiat Oncol Biol Phys 2000;48:1381-7. Back to cited text no. 19 [PUBMED] [FULLTEXT] |
| 20. | Kalapurakal JA, Silverman CL, Akhtar N, Andrews DW, Downes B, Thomas PR. Improved trigeminal and facial nerve tolerance following fractionated stereotactic radiotherapy for large acoustic neuromas. Br J Radiol 1999;72:1202-7. Back to cited text no. 20 [PUBMED] [FULLTEXT] |
| 21. | Meijer OW, Wolbers JG, Baayen JC, Slotman BJ. Fractionated stereotactic radiation therapy and single high-dose radiosurgery for acoustic neuroma: Early results of a prospective clinical study. Int J Radiat Oncol Biol Phys 2000;46:45-9. Back to cited text no. 21 [PUBMED] [FULLTEXT] |
| 22. | Hanks GE, Hanlon AL, Schultheiss TE, Pinover WH, Movsas B, Epstein BE, et al. Dose escalation with 3D conformal treatment: Five-year outcomes, treatment optimization and future directions. Int J Radiat Oncol Biol Phys 1998;41:501-10. Back to cited text no. 22 [PUBMED] [FULLTEXT] |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04075f1.jpg]
|

{kind=link}