 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 251-253 Case Report Subarachnoid spread of germinoma mimicking tuberculous meningitis Suresh TN, Mahadevan Anita , Santosh Vani , Shankar SK Department of Neuropathology, National Institute of Mental Health and Neurosciences, Bangalore - 560029
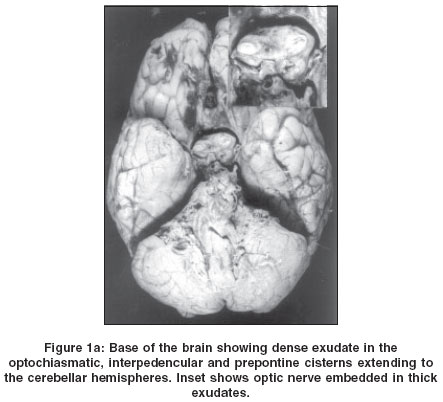
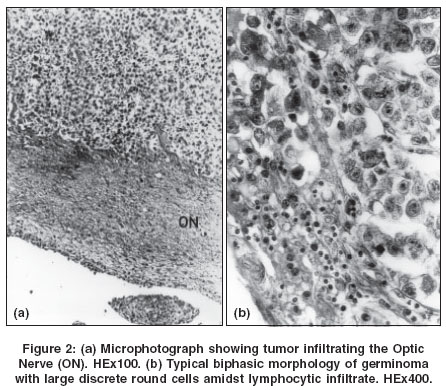
Correspondence Address:Department of Neuropathology, NIMHANS, Bangalore - 560029 Code Number: ni04076 Abstract A case of pineal germinaoma spreading along the basal subarachnoid space, clinically and macroscopically at autopsy, resembling tuberculous basal arachnoiditis is reported. Need to carry out CSF cytology of even hemorrhagic CSF is stressed, to diagnose the condition. Keywords: Germinoma, tuberculous meningitis, basal meningitis Introduction Germ cell tumors (GCT) arising primarily in the central nervous system are rare and constitute only a small fraction of all intracranial tumors. Germinomas are the most common of the GCTs with suprasellar being the most common site.[1] Compression of the adjoining neuroanatomical structures by these tumors accounts for their common modes of presentation with features of raised intracranial tension, visual deficits and neuroendocrine symptoms. Though germinomas are notorious for their propensity to spread into the CSF pathways, primary presentation with features of CSF dissemination along the basal cisterns is extremely rare. This case report illustrates one such case wherein the signs and symptoms caused by the dense subarachnoid dissemination of the tumor were so prominent as to mimic a basal meningitis not just clinically but even on gross examination of the brain at postmortem. Only histopathological examination exposed the true neoplastic nature of the lesion and the disease process. Case Report A 23-year-old lady presented with a low-grade intermittent fever for the last two months and associated progressive dimness of vision affecting the right eye more than the left. But over the last ten days she developed headache and vomiting and soon lapsed into a delirious state, talking irrelevantly and failing to recognize her own relatives. On admission, she was found to be pale, withdrawn, listless and disoriented. Physical examination, except for a few firm, non-matted lymphnodes in the submandibular region, was not contributory. Examination of the nervous system showed signs of meningeal irritation. Optic fundoscopy revealed primary optic atrophy on the right. Both pupils were equal and reactive to light. No sensory or motor deficits were present. Cranial nerves, except for the left upper motor neuron facial palsy, were unaffected. Visual fields could not be tested as the patient was non-cooperative. A lumbar puncture drew uniformly blood-stained CSF fluid under raised pressure. The protein content was 70 mg% and sugar 40 mg%. The large number of RBCs precluded a cell count. The lumbar punctures, repeated on two more occasions were again hemorrhagic. The cell count on one occasion was reported to be 20 cells/mm3 (all lymphocytes). In view of hemorrhagic CSF, the possibility of subarachnoid hemorrhage secondary to aneurysmal leak was considered. A right carotid angiogram with cross compression did not reveal any aneurysm. A conray ventriculogram showed dilatation of the right lateral ventricle. The foramen of Munroe was patent and the dye was seen to fill the aqueduct and the fourth ventricle. But the anterior third ventricle showed filling defects. The patient′s sensorium deteriorated necessitating a ventriculoperitoneal shunt. The ventricular CSF was also blood-stained. Post-procedure, the patient improved but two weeks later she developed pain radiating from the vertex along the shunt tube with extravasation of CSF requiring shunt revision. Subsequently, a diagnostic open biopsy was attempted through a frontal craniotomy. At surgery, both optic nerves and chiasma were noted to be enlarged and entrapped by abnormal looking tissue which was biopsied and sent for histopathological examination. Tissue diagnosis was inconclusive due to inadequate biopsy. Unfortunately, within a couple of hours post surgery, the patient succumbed. A partial autopsy confined to the removal of the brain was carried out. On external examination, a blood clot was seen covering the site of the burr hole over the right frontal lobe. A striking finding was a thick, dense organized exudate seen filling the chiasmatic, interpeduncular, pontine cisterns along the base of the brain and entrapping the cranial nerves and cerebral vessels [Figure - 1]a). The optic nerves were embedded within the exudate that was seen to track laterally along both sylvian fissures while posteriorly encasing the brainstem, pons, medulla and cerebellum, obliterating the lateral foramina of the fourth ventricle. Examination of the coronal slices revealed hemorrhagic softening of the right caudate nuclei, putamen and the anterior limb of the internal capsules. The ventricular system was dilated. The right frontal horn was filled with blood clots while the left was filled with necrotic material. The ependymal lining of the ventricles was shaggy. A large hemorrhagic mass was noted in the anterior third ventricle, continuous with the basal subarachnoid space [Figure - 1]b). Histopathological examination of the sections from the basal ganglia and hypothalamus showed a large tumor mass that was cystic and hemorrhagic. The mass occupied the anterior and middle third of the third ventricle, infiltrating the hypothalamus, columns of fornix and extending anteriorly into the optic chiasma and optic nerve entering the orbital foramina. The ependymal lining of the third ventricle and choroid plexus were bathed in an acute inflammatory exudate. Tumor seedlings were seen in the temporal horn of the lateral ventricle and the head of the caudate nucleus. The optic nerve was enveloped and infiltrated by the tumor, forming segmented cords and islands disrupting the nerve fibers [Figure - 2]a). The tumor cells were seen spilling into the subarachnoid space to cover the ventral aspect of the brainstem. Tumor implants were identified within the medulla near the floor of the fourth ventricle infiltrating the lower cranial nerve nuclei. The pineal gland was totally replaced by the tumor leaving behind only the capsule and concentric calcific bodies to identify the gland. Histomorphologically, the tumor was moderately vascular and had the typical biphasic morphology of a germinoma with large round discrete cells amidst a lymphocytic infiltrate [Figure - 2]b). The cerebral cortex and cerebellum did not have tumor infiltrate though the surface subarachnoid had occasional germinoma cells. The tumor cells were monomorphic, infiltrating into the brain as lobular masses. Some of the parenchymal and subarachnoid vessels had tumor emboli. The tumor was mitotically active. No areas suggestive of syncytio/cytotrophoblastc components were noted. Discussion Germinomas are the most common of the intracranial germ cell tumors. At our Institute, among a total of 6353 intracranial tumors seen over the last 15 years, 25 (0.4%) were germ cell tumors (GCTs) . Germinomas of the nervous system constituted 72%(18) of GCTs. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04076f2.jpg] [ni04076f1b.jpg] [ni04076f1a.jpg] |
| |||||||||

{kind=link}
![Figure - 1]b](/showimage?ni/photo/ni04076f1b.jpg){kind=link}
{kind=link}