
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 259-260
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 259-260
Case Report
Giant intraparenchymal neurocysticercosis: Unusual MRI findings
Agarwal Prachi P, Gaikwad Shailesh B, Garg Ajay , Gupta Vipul , Mishra NK, Mehta VS
Departments of Neuroradiology, Neurosciences Centre, All India Institute of Medical Sciences, New Delhi - 110029
Correspondence Address:Department of Neuroradiology, AIIMS, New Delhi-110029
sgaikwad_63@yahoo.com
Code Number: ni04079
Abstract We report a case of surgically proven giant neurocysticercosis (NCC). MR imaging revealed an unusually large solitary parenchymal cystic lesion showing signal intensity similar to CSF on all pulse sequences, with internal septations and a small nodule in the anterior aspect of this lesion compatible with this diagnosis. Identification of a scolex in a cystic lesion with CSF intensity plays a key role in the diagnosis of NCC. The presence of internal septations is an atypical feature.
Keywords: Neurocysticercosis, parasitic infection
Introduction Neurocysticercosis (NCC) is a common CNS parasitic infection worldwide, affecting humans as intermediate hosts in the lifecycle of Taenia solium, when they ingest eggs from contaminated food.[1] The diagnosis of NCC often depends on a combination of clinical symptoms, CSF analysis and radiological findings.[2] Giant NCC is a rare condition defined by various authors as measuring more than 4 or 5 cm in its largest dimension.[3] The MR imaging appearances of NCC and its pathological correlation are well described.[4],[5] We report the MRI findings in a rare case of surgically proven giant NCC and describe MR features, which may suggest the diagnosis. Case Report
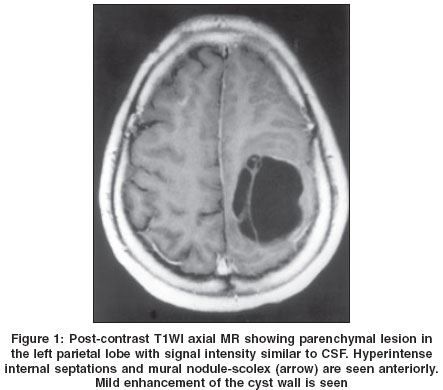
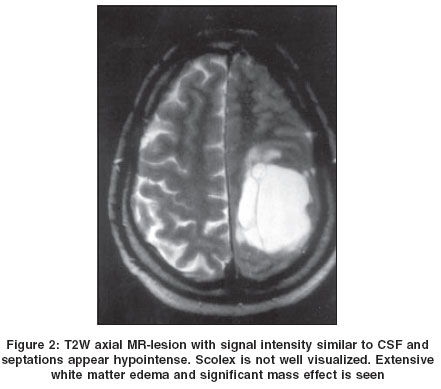
A 50 year old right-handed male had a one-year history of headaches and had a seizure 4 months. On examination, he had right-sided hemiparesis (power Grade 4/5 in right upper and lower limbs). Contrast-enhanced CT demonstrated a large cystic lesion in the left parietal lobe with compression of the ipsilateral lateral ventricle and displacement of midline structures to the right. The cyst had density similar to the CSF with internal septations and perifocal edema. There was no enhancement or calcification. MR scan confirmed the sharply demarcated 5.5 cm x 4 cm x 5.5 cm cystic lesion. The signal intensity of the cyst was similar to CSF in all sequences. The multiple septae were hyperintense on T1WI [Figure - 1] and hypointense on T2WI [Figure - 2].
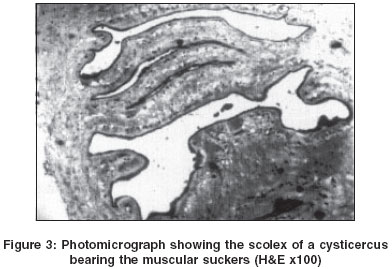
The cyst had a thin smooth wall, which was hypointense on T2WI. In addition, a single mural nodule (scolex-arrow) was seen anteriorly in the axial plane with minimal enhancement on T1WI post contrast images . The scolex was not clearly visualized on T2WI. The cyst was surrounded by high signal edema along white matter on T2WI. At surgery, a single large parenchymal cyst was found with scolex attached to the anterior wall and cyst fluid was clear. Histopathogy confirmed the diagnosis of NCC [Figure - 3].Discussion Human cysticercosis occurs when man serves as an incidental intermediate host to Taenia solium, the pork tapeworm. Imaging plays a crucial role in the diagnosis of this neuroparasitosis. CNS involvement occurs in 60-90% of patients with cysticercosis.[6] Five forms of NCC have been recognized depending on location, namely parenchymal, arachnoidal, ventricular, spinal and mixed.[7] Imaging findings correlating to four stages have been well described by Escobar.[5]
However, as degeneration begins, the host response ensues resulting in edema and cyst wall enhancement. In our case, the cysticercus was in this stage. Also, the cystic fluid becomes more turbid (colloidal vesicular stage). In the granular nodular stage, the cyst retracts with thickening of the capsule producing a ′white target′ appearance on T2WI with edema appearing as hyperintense and capsule and scolex demonstrating low signal in the center. In the final stage (nodular calcified stage) the lesion contracts to a fraction of its initial size and is completely mineralized. A ′black target′ appearance is seen on T2WI due to marked T2 shortening which may reflect the presence of calcification, collagen, petechial hemorrhage and/or free radicals produced by macrophages. A central high-intensity dot may be due to a small amount of cystic fluid rather than scolex.
In the present case the cysticercus appeared to be in the early degenerating stage because it showed perifocal edema and mild enhancement of its capsule. The typical size of cysticercus cellulosae is 1 cm (ranging from 4-20 mm in diameter).[8] This case was an unusually large cyst measuring 5.5 cm x 4 cm x 5.5 cm. Another atypical feature was the presence of internal septae. A cysticercus is known to have only one bladder with no septations. To the best of our knowledge, septations have been previously described in only one case in English literature, which proved to be a single cyst on surgery.[1] In a single cyst folding of the cyst wall may explain the internal septations.[1] However, multiple conglomerate cysts may also manifest like this. Cysticercal cysts in the basal cisterns tend to agglomerate in a racemose form[9] and these cysts usually lack a scolex.[10] Trelles et al[11] suggest that disordered proliferation of the cyst wall is associated with the disappearance of scolex while Martinez[12] holds that the racemose cysts are an arrested form in the development of the cyst, the scolex never being formed. Also, Bickerstaff et al[13] suggest that the racemose form develops because in the basal cisterns there is no limiting host response of encapsulation, such as happens in the parenchymal form. In our case, on surgery, a single large parenchymal cyst was found with scolex attached to the anterior wall. We believe that folding of the cyst wall gave the appearance of septations in MR imaging. Pathognomonic imaging characteristics (i.e. the presence of scolex within a cystic lesion) permit the diagnosis to be made.[9] MRI has a higher sensitivity in detecting scolex compared to CT as also exemplified in our case. Despite the unusually large size and internal septae, the presence of scolex gave a clue to the correct diagnosis. However, scolex may not be detected even by MRI in all cases depending on their size, slice thickness of MRI and direction of section plane.[1] The differential diagnosis for this lesion would include necrotic cystic tumor, hydatid cyst and porencephalic cyst. MRI can differentiate between these lesions by demonstrating scolex. Also, the signal intensity of the contents of cystic tumors differs from that of CSF and a hydatid cyst is expected to be more spherical. A porencephalic cyst does not show perilesional edema or mass effect as seen in this case. Besides, enhancement is not a feature of a porencephalic cyst.
References
| 1. | Suh DC, Chang KH, Han MH, Lee SR, Han MC, Kim CW. Unusual MR manifestations of neurocysticercosis. Neuroradiology 1989;31:396-402. Back to cited text no. 1 [PUBMED] |
| 2. | Suss RA, Maravilla KR, Thomson J. MR imaging of intracranial cysticercosis: Comparison with CT and anatomopathologic features. AJNR Am J Neuroradiol 1986;7:235-42. Back to cited text no. 2 |
| 3. | Colli BO, Martelli N, Assirati JA Jr, et al. Surgical treatment of cysticercosis of the central nervous system. Neurosurgery Quarterly 1995:5;34-5. Back to cited text no. 3 |
| 4. | Teitelbaum GP, Otto RJ, Lin M, Watanabe AT, Stull MA, Manz HJ, et al. MR imaging of neurocysticercosis. AJNR Am J Neuroradiol 1989;10:709-18. Back to cited text no. 4 |
| 5. | Escobar A. The pathology of neurocysticercosis of the central nervous system. In: Palacios E, Rodriguez-Carbajal J, Taveras JM, (Ed). Cysticercosis of the central nervous system. Springield, IL: Charles C Thomas 1983:27-54. Back to cited text no. 5 |
| 6. | Chang KH, Cho SY, Hesselink lin JR, et al. Parasitic diseases of the central nervous system. Neuroimaging Clin N America 1991;1:159-78. Back to cited text no. 6 |
| 7. | Palacios E, Lujambio PS, Jasso RR. Computed Tomography and magnetic resonance imaging of neurocysticercosis. Semin in Roentgen 1997;32:325-34. Back to cited text no. 7 |
| 8. | Martinez HR, Gurra RR, Elizondo G, Gonzalez J, Todd LE, Ancer J, et al. MR imaging in neurocysticercosis: A study of 56 cases. AJNR Am J Neuroradiol 1989;10:1011-9. Back to cited text no. 8 |
| 9. | Zee CS, Go JL, Kim PE, DiGiorgio CM. Imaging of neurocysticercosis. Neuroimaging Clin N America 2000;10:391-407. Back to cited text no. 9 |
| 10. | McCormick GF, Zee CS, Heiden J. Cysticercosis cerebri: Review of 127 cases. Arch Neurol 1982;39:534-9. Back to cited text no. 10 [PUBMED] |
| 11. | Trelles JO, Rocca E, Ravens R. Estudios sobre neurocisticercosis: Sobre la fina estructura de la membrana vesicular quistica y racemosa-deducciones pathologicas. Rev Neuropsiquist 1952;15:1-35. Back to cited text no. 11 |
| 12. | Martinez A. Anatomica pathologica de la cisticercosis cerebral. Neurocirugia 1961;19:191-201. Back to cited text no. 12 |
| 13. | Bickerstaff Er, Small JM, Woolf AL. Cysticercosis of the posterior fossa. Brain 1956;79:622-34. Back to cited text no. 13 [PUBMED] |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04079f1.jpg]
[ni04079f2.jpg]
[ni04079f3.jpg]
|

{kind=link}
{kind=link}
{kind=link}