 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
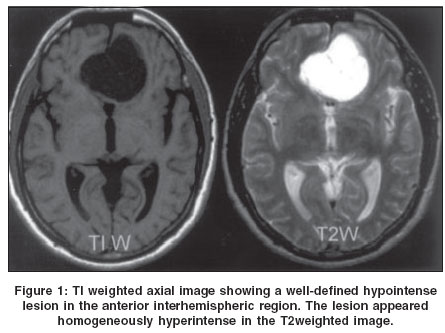
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 261-262 Short Reports Cystic olfactory groove schwannoma Shenoy SN, Raja A Department of Neurosurgery, Kasturba Medical College and Hospital, Manipal
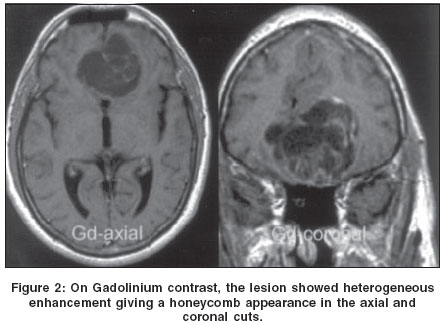
Correspondence Address:Department of Neurosurgery, Kasturba Medical College and Hospital, Manipal - 576119. Udupi Code Number: ni04080 Abstract Intracranial schwannoma not related to cranial nerves are unusual and rarely found in the subfrontal region. We report a case of cystic olfactory groove schwannoma in a 55-year- old male, who presented with late onset seizure without raised intracranial pressure. The tumor was excised completely.Keywords: Schwannoma, anterior cranial fossa, neurilemmoma Introduction Intracranial schwannomas not associated with cranial nerves account for less than 1% of surgically treated schwannomas of the central and peripheral nervous system.[1],[2] Subfrontal schwannomas are rare and less than 20 cases have been reported in the literature.[1],[2],[3],[4],[5] We report a case of cystic olfactory groove schwannoma and briefly review the literature. Case Report A 55-year-old man had an episode of generalized seizures. There were no symptoms of raised intracranial pressure or focal neurological deficit. Neurological examination revealed preserved olfaction and no other abnormality. The T1-weighted magnetic resonance (MR) image revealed a well-defined hypointense lesion situated in the midline anterior cranial fossa, elevating and minimally compressing the frontal lobe. The lesion was homogenously hyperintense in the T2-weighted image and isointense in the flair images [Figure - 1]. The Gadolinium injection caused a heterogeneous enhancement giving it a honeycomb appearance [Figure - 2]. He underwent left fronto-temporal craniotomy and total excision of the tumor. The tumor was grayish, well-defined and contained multiple cysts filled with xanthochromic fluid. The intervening tissue was grayish, containing thin blood vessels. The tumor was attached to the dura just lateral to the left cribriform plate with a narrow pedicle. The ipsilateral olfactory bulb was flattened and markedly thinned out and could not be separated from the surrounding gliotic cortex. However, the contralateral olfactory tract was preserved. The histopathological features were suggestive of typical schwannoma. The tumor cells exhibited a strongly positive staining pattern for S-100 protein. Discussion Schwannomas commonly arise from the nerve sheaths of the peripheral and the cranial nerves and represent approximately 8% of all intracranial tumors.[5] Even though schwannomas have been reported to originate from all the cranial nerves, except the optic nerve, most arise from the vestibular nerve.[5] Very few cases of intracranial schwannomas without a cranial nerve or dural attachment have been reported in the literature.[1],[2],[3],[4] The pathogenesis of these intracranial schwannomas is puzzling as the central nervous system is devoid of the Schwann cells.[1],[2] Various theories regarding the possible origin of these tumors are centered around developmental and non-developmental origins.[1],[2],[5] The developmental theories suggest either transformation of mesenchymal pial cells into ectodermal Schwann cells or migration of the neural crest cells within the substance of the central nervous system.[5] On the other hand, the proponents of the non-developmental theories postulate that intracranial schwannomas arise from Schwann cells normally present in the adjacent structures such as the perivascular nerve plexus and the meningeal branches of the trigeminal and anterior ethmoidal nerves innervating the anterior cranial fossa.[5] In our case, the tumor was arising from the basal dura at the site of olfactory bulb. The attachment of the tumor was very narrow, suggesting that the schwannoma might have originated from the small nerves in the basal dura matter. References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04080f1.jpg] [ni04080f2.jpg] |
| |||||||||

{kind=link}
{kind=link}