 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
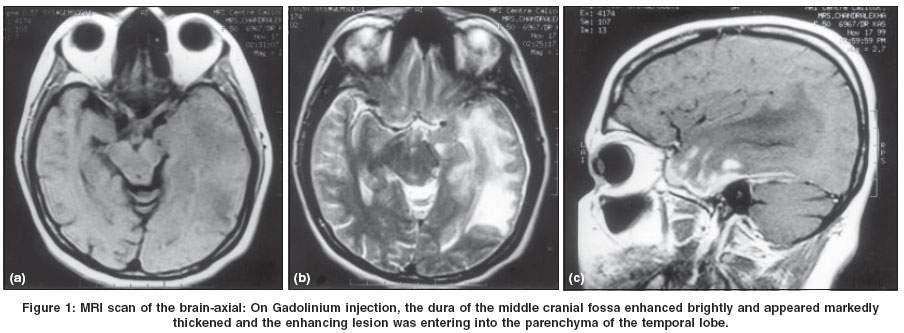
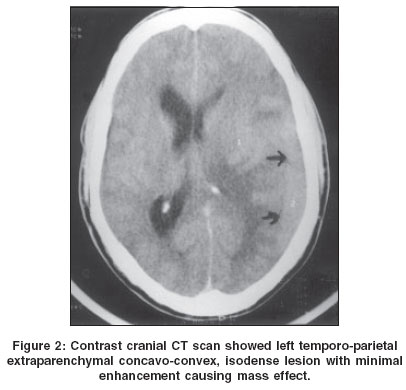
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 262-264 Short Reports Intracranial plasma cell granuloma Shenoy SN, Raja A Department of Neurosurgery, Kasturba Medical College and Hospital, Manipal
Correspondence Address:Department of Neurosurgery, Kasturba Medical College and Hospital, Manipal - 576119, Udupi Code Number: ni04081 Abstract We report two rare cases of primary intracranial plasma cell granuloma. The tumors probably arose from the dura and involved the cerebral parenchyma. These patients presented with clinical features of raised intracranial pressure and there was focal neurological deficit. The management issues are discussed.Keywords: Inflammatory pseudotumor, plasma cell granuloma Introduction Plasma cell granuloma (PCG) is a rare form of idiopathic inflammatory pseudotumor, characterized by a benign proliferation consisting predominantly of plasma cells and reticuloendothelial elements.[1] Very few cases of primary PCG of the central nervous system are reported.[2],[3],[4] We describe two cases of primary intracranial PCG and briefly discuss the literature on the subject. Case Reports Case 1 A 48-year-old lady was admitted with history of progressively worsening headache for one month. She had bilateral early papilledema and no other focal neurological deficit. A CT scan revealed an isodense non-enhancing diffuse left temporal lesion causing mass effect. T1-weighted MRI revealed a diffuse hypointense lesion and T2-weighted MRI revealed a hyperintense lesion in the left temporal lobe. The lesion showed heterogeneous contrast enhancement [Figure - 1]. She underwent left temporal craniotomy and excision of the lesion. The lesion was dura-based and infiltrated the underlying brain. The brain was edematous. Histopathological examination showed chronic inflammatory infiltration of the dura, mainly with plasma cells and a few lymphocytes and histiocytes. A few Russell bodies were present. Her investigations for plasma cell dyscrasias were negative. At 36 months follow-up the patient was asymptomatic. Case 2 Discussion The term "plasma cell granuloma" is used to describe a localized benign proliferation of mature plasma cells.[1] Only a few cases of primary PCG of the central nervous system have been reported.[2],[3],[4] Plasma cell granulomas are known to arise from the meninges, sella, choroid plexus, fourth ventricle, and hypothalamic region.[2],[3],[4] Radiologically, the differential diagnosis of PCG includes en plaque meningioma and granulomas. Similarly, it should be differentiated histologically from plasmacytoma and meningioma with plasma cell infiltrate.[5],[6] Solitary intracranial plasmacytoma is a rare neoplastic lesion characterized by typical monoclonal plasma cells.[6] Horten et al reported cases, which revealed mixed populations of proliferating meningothelial cells together with plasma cells and lymphocytes.[5] References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04081f1.jpg] [ni04081f2.jpg] |
| |||||||||

{kind=link}
{kind=link}