 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 264-265 Short Reports Intramedullary cysticercosis Singh Prakash , Sahai K Army Hospital (R&R), Delhi Cantt - 110010
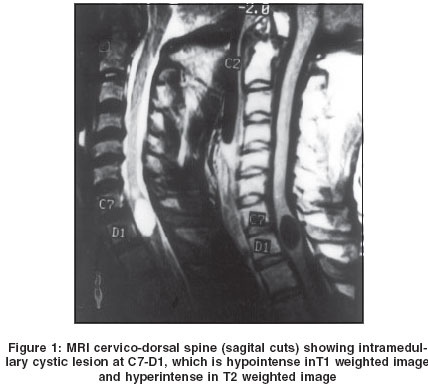
Correspondence Address:Neurosurgeon, Army Hospital (R&R) Delhi Cantt-110010 Code Number: ni04082 Abstract A 42-year-old soldier, a known case of cerebral parenchymal neurocysticercosis presented with insidious onset gradually progressive weakness of both lower limbs for six months. Investigations revealed an intramedullary cyst in the cervicodorsal region. Following surgical excision of an intramedullary cysticercus cyst, the patient showed recovery in his neurological deficits.Keywords: Intramedullary tumor, cysticercosis Introduction Intramedullary cysticercosis is a rare manifestation of neurocysticercosis.[1],[2],[3],[4] We report a case and briefly review the literature on this subject. Case Report A 42-year-old man had a generalized seizure 2 years back. He was investigated with computerized tomography (CT) scan of brain and was diagnosed to have cerebral neurocysticercosis. He was treated with albendazole (15mg / kg body weight) for four weeks in addition to anticonvulsant drugs. He now presented with history of insidious onset, gradually progressive weakness of the lower limbs of six months duration. The weakness started with the right leg. For one month he had urinary hesitancy. At the time of presentation he could walk only with support. Neurological evaluation revealed spastic Grade 4 paraparesis and the sensory level was at T3 dermatome. MRI of the cervicodorsal spine revealed an intramedullary cystic lesion at C7-T1, which was hypointense in T1- weighted images and hyperintense in T2-weighted images [Figure - 1] and did not enhance after gadolinium contrast administration. A few cysts in the cervical musculature were also noted. MRI of brain revealed some persisting parenchymal cysts. The patient was subjected to C7 to D2 laminectomy. The spinal cord was enlarged at this level and through right dorsal root entry zone myelotomy, a well-circumscribed grayish white cyst was seen under the operating microscope and was completely removed. The postoperative period was uneventful. Histological examination showed cyst wall thrown into folds enclosing body cavity of the parasite. At places scolex and hooklets could be identified thus confirming the diagnosis of cysticercus. No calcareal corpuscles or pericystic inflammation was seen. He was given another course of albendazole (15 mg/kg body weight) for four weeks. He gradually improved and at 3-months follow-up, except for brisk deep tendon reflexes in the lower limbs, had no other deficit. Postoperative MRI confirmed the complete resolution of cystic lesion. Discussion Cysticercosis is a common infestation of the central nervous system. Spinal involvement is rare and varies from 0.7 to 5.85%.[5],[6],[7] Spinal forms have been identified in the vertebral, extradural, intradural and intramedullary regions. Intramedullary cysticercosis is very uncommon and only 45 cases have been reported so far.[1],[8] Migration of the cysticercus through the ventriculo-ependymal pathway and hematogeneous dissemination have been identified to be the possible pathogenetic mechanisms. The higher incidence in the thoracic spinal cord is possibly related to the high blood flow in the thoracic segment of the spinal cord.[1],[5],[9] In the absence of previous history of neurocysticercosis or subcutaneous nodules it may be difficult to clinically suspect intramedullary cysticercosis. High eosinophil count and calcification of soft tissues in the plain radiogram may be suggestive, but such findings are rare.[1],[10] Cerebrospinal fluid and serum enzyme-linked immunoelectric transfer blot assay for cysticercus antibodies may be helpful.[11] MRI clearly delineates the lesion. Concurrent presence of cerebral and muscular cysticercosis in the presence of spinal cysticercosis has been reported.[12],[13] Results of surgery have not been encouraging till a decade back[8],[9] and this has been attributed to parenchymal gliosis as result of toxic waste products of larva, pachymeningitis and vascular insufficiency.[2],[5],[8] However, in the microsurgical era, good surgical outcome has been reported.[1],[13] References
Copyright 2004 - Neurology India The following images related to this document are available:Photo images[ni04082f1.jpg] |
| |||||||||

{kind=link}