
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 265-267
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 265-267
Short Reports
New solitary cysticercus granulomas causing recurrent symptoms in patients with resolved solitary granulomas
Sujit Kumar GSamson , Rajshekhar Vedantam
Department of Neurological Sciences, Christian Medical College and Hospital, Vellore
Correspondence Address:Department of Neurological Sciences, Christian Medical College and Hospital, Vellore - 632004
Code Number: ni04083
Abstract Recurrence of symptoms in a patient with a resolved solitary cerebral cysticercus granuloma (SCCG) is uncommon. Recurrent seizures in these patients are generally attributed to an epileptogenic scar or calcific residue of the granuloma. We report two patients with recurrent seizures and one patient with headache; all three patients were previously diagnosed to have SCCG and had complete resolution of the granuloma on follow-up imaging. Computed tomography (CT) at the time of recurrent symptoms showed a SCCG at a site different from the initial lesion, but in the same cerebral hemisphere in all the three patients. Since a new lesion can cause recurrent symptoms in patients with a resolved SCCG, repeat imaging should be performed in all these patients. We also postulate that recurrent cysticercal lesions in patients who have previously had a SCCG, tend to be solitary.
Keywords: Neurocysticercosis, epilepsy, computed tomography
Introduction Solitary cerebral cysticercus granuloma (SCCG) is a common cause of seizures in endemic areas like India.[1] These granulomas usually resolve spontaneously with either complete disappearance or with a calcific residue. Nearly 70 % of SCCGs show some degree of resolution within six months of presentation.[2] Recurrence of seizures can occur in some patients with SCCG even after complete resolution of the granuloma. Recurrent symptoms are usually attributed to a calcific residue[3] or an epileptogenic scar. We report two patients with recurrent seizures and one with severe headache, all of whom had a resolved SCCG. A fresh SCCG at a location different from the initial site in all the three patients was demonstrated as the cause of the recurrent symptoms. Case Reports
Patient 1
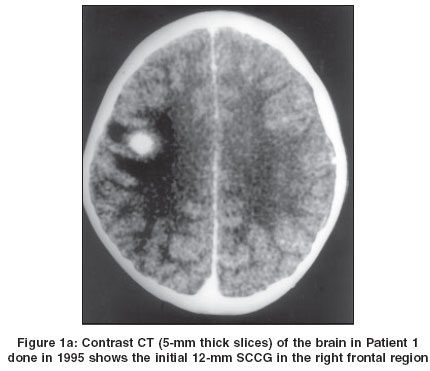
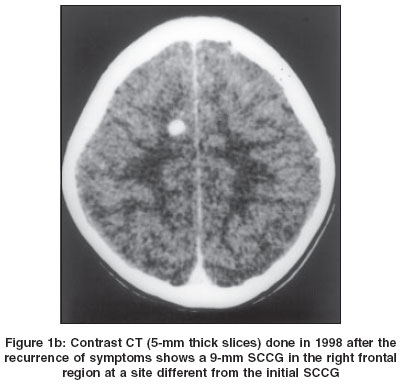
A 7-year-old girl presented with left facial focal motor seizures in September 1995. CT at initial presentation showed a 12 mm disc lesion in the right posterior frontal region with perilesional edema [Figure - 1]a. She was treated with antiepileptic drugs (AEDs) for a two-year period and then they were tapered over a period of six months. She was asymptomatic till February 1998 when she developed left upper limb focal motor seizures. A CT at this time showed a 9 mm granuloma in the right frontal region with perilesional edema, at a site different from the previous SCCG [Figure - 1]b. The previous SCCG was seen to have resolved completely.Patient 2
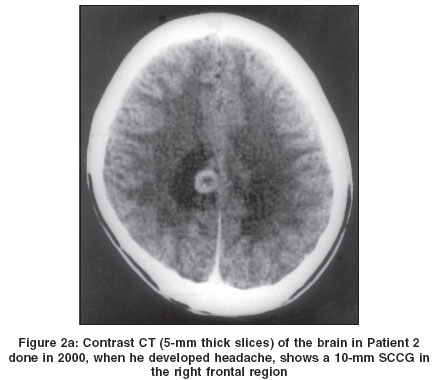
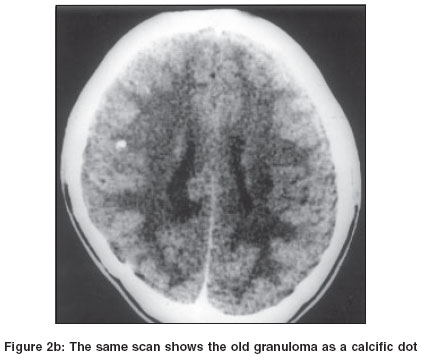
A 10-year-old boy presented with left facial focal motor seizures in February 1993. CT of the brain at that time showed a right frontal SCCG with perilesional edema. He was treated with AEDs for two years after which they were tapered off. He was asymptomatic till September 2000 when he reported one episode of severe headache. CT showed a right frontal 10 mm SCCG with perilesional edema [Figure - 2]a. The old lesion was seen as a calcific dot [Figure - 2]b. He was advised symptomatic therapy with regular follow-up monitoring. Patient 3
This case has been reported earlier.[4] A 4-year-old boy was diagnosed to have SCCG in April 1994. CT of the brain at that time showed a 10 mm ring-enhancing lesion in the left parietal region with perilesional edema. He was treated with AEDs and a repeat CT in November 1994 revealed a tiny residue of the granuloma. The AEDs were tapered over the next six months. He was asymptomatic till February 1998 when he developed right focal seizures with secondary generalization. CT showed a 10 mm contrast-enhancing lesion in the left parietal region anterior to the location of the initial SCCG, which was seen as a calcific residue. Discussion In our second and third patients a new lesion was seen distinct from the initial lesions and the old lesions were seen as calcific dots. In the first patient, the comparison of the initial scan and the scan done during recurrence of symptoms showed that the granulomas were located at different sites. In our patients, the new lesions and not the residue of the first granulomas, were clearly the causes of the recurrent symptoms as they were associated with perilesional edema indicating that they were immunologically active.
Interestingly, the new lesions in all our patients were again solitary lesions. This suggests that in a patient who previously had a SCCG, neurocysticercosis is likely to manifest with a solitary lesion rather than with multiple lesions. This could be due to a unique host-parasite interaction based on the individual′s immunity and parasite-dependent factors or it could be related to the parasite load. In all three patients the new lesion occurred on the same side as the initial granuloma. The cause for this is unclear but as the parasite reaches the brain hematogenously, it is possible that cerebral hemodynamic factors unique to each of these patients ensured that the parasitic emboli were preferentially carried to one cerebral hemisphere. We postulate that all the new granulomas in our patients resulted from reinfection. It is possible that the new granuloma was the result of the initial infection. A live cyst from the initial infection might not have been visualized in the first scan as it was small and non-enhancing. Subsequent degeneration of the live cyst could have led to inflammation and enhancement with visualization on a CT scan. But this is a less likely explanation as there was an interval of 2.5, 4 and 7.5 years between the presentation of the two granulomas. One would expect that the degeneration of cysts from the same infection would not be temporally separated by such long intervals of time.
Reappearance of a SCCG at the same site after documented "resolution" was previously described by other authors.[5],[6],[7] The reappearance of the granuloma in these patients almost always coincided with recurrence of symptoms which prompted a repeat imaging of the brain. We postulated that lack of adequate contrast injection or thick CT slices (>5 mm) in the follow-up CT scan could have led to a false positive diagnosis of "disappearance" of the granuloma.[8]
The treatment for patients with recurrent seizures and a new SCCG is the same as that for the initial lesion. Therefore these patients were managed conservatively and the AEDs were stopped after the resolution of the new lesion. We decided to follow up the second patient and did not restart him on AEDs. In a previous study, we found that 14/15 patients who presented with severe episodic headache due to SCCG, did not develop seizures on follow-up.[9]
In conclusion, we recommend a repeat imaging in a patient with a resolved SCCG who presents with recurrent or new symptoms, even if the recurrent symptoms are similar to the initial symptomatology and can be explained by the location of the initial granuloma. A new lesion should be actively sought in these patients′ images. We postulate that when new lesions occur in patients with a SCCG they tend to be solitary rather than multiple and recommend that the management strategy for the new SCCG be the same as that used for the initial granuloma.
References
| 1. | Rajshekhar V. Etiology and management of single small enhancing CT lesion in patients with epilepsy. Understanding a controversy. Acta Neurol Scand 1991;84:565-70. Back to cited text no. 1 |
| 2. | Rajshekhar V. Rate of spontaneous resolution of a solitary cysticercus granuloma in patients with seizures. Neurology 2001;57:2315-7. Back to cited text no. 2 [PUBMED] |
| 3. | Murthy JMK, Reddy YVS. Prognosis of epilepsy associated with single CT enhancing lesion: A long term follow up study. J Neurol Sci 1998;159:151-5. Back to cited text no. 3 |
| 4. | Rajshekhar V. Recurrent seizures in a patient with a calcified solitary cysticercus granuloma caused by a fresh solitary granuloma. Ann Ind Acad Neurol 1999;2:25-7. Back to cited text no. 4 |
| 5. | Goulatia RK, Verma A, Misra NK, et al. Disappearing CT lesions in epilepsy. Epilepsia 1987;28:523-7. Back to cited text no. 5 |
| 6. | Sethi PP, Wadia RS, Kiyawat DP, et al. Ring or disc enhancing lesions in epilepsy in India. J Trop Med Hyg 1994;97:347-53. Back to cited text no. 6 [PUBMED] |
| 7. | Ahuja GK, Behari M, Prasad K, et al. Disappearing CT lesions in epilepsy: Is tuberculosis or cysticercosis the cause? J Neurol Neurosurg Psychiatry 1989;52:915-6. Back to cited text no. 7 [PUBMED] |
| 8. | Rajshekhar V, Abraham J. Disappearing CT lesions in Indian patients with epilepsy. J Neurol Neurosurg Psychiatry 1990;53:818. Back to cited text no. 8 [PUBMED] |
| 9. | Rajshekhar V. Severe episodic headache as the sole presenting ictal event in patients with a solitary cysticercus granuloma. Acta Neurol Scand 2000;102:44-6. Back to cited text no. 9 [PUBMED] [FULLTEXT] |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04083f1b.jpg]
[ni04083f2b.jpg]
[ni04083f1a.jpg]
[ni04083f2a.jpg]
|

{kind=link}
{kind=link}
{kind=link}
{kind=link}