
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 272-273
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 272-273
Letter To Editor
Non-traumatic atlantoaxial rotatory subluxation
Shenoy SN, Raja A
Department of Neurosurgery, Kasturba Medical College and Hospital, Manipal
Correspondence Address:Department of Neurosurgery, Kasturba Medical College and Hospital, Manipal
shenoysn@yahoo.com
Code Number: ni04090
Sir,
A 17-year-old girl presented with complaints of sudden onset of torticollis associated with severe neck pain and restriction of neck movements. There was no history of trauma. On examination, she had "cock robin" deformity of the head, which was rotated to the left and the chin was directed to the right side. There was no neurological deficit.
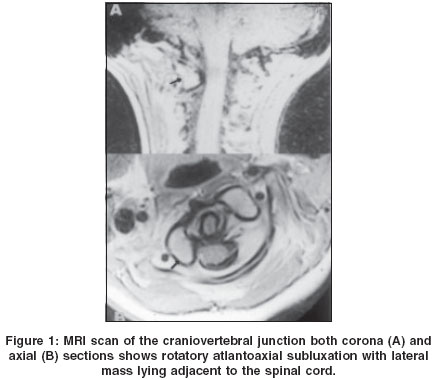
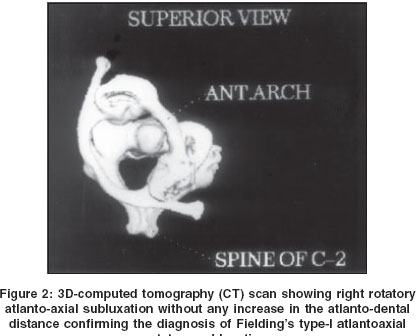
X-ray of the craniovertebral junction (CVJ) (open mouth view) revealed overlapping of the lateral masses causing obscuration of the lateral atlantoaxial joints. Magnetic resonance imaging (MRI) scan of the cervical spine revealed rotatory subluxation of the atlas with the lateral mass lying adjacent to the cord [Figure - 1]. 3D-computed tomography (CT) scan revealed Fielding′s Type I atlantoaxial rotatory subluxation[2] [Figure - 2]. She was treated with Gardner-Well′s skull traction and reduction was achieved. Dynamic CT scan revealed adequate reduction of the atlantoaxial rotatory subluxation. However, at the end of two weeks, she returned with torticollis despite wearing the cervical collar. She was again treated with Gardner-Well′s traction for two weeks followed by cervical collar for three months. At 42 months follow-up, she was asymptomatic.
Rotatory atlantoaxial subluxation is an uncommon and poorly understood clinical entity.[1] Various conditions which can predispose to rotatory subluxation include inflammation, and surgical procedures in and around the throat, neck and cervical spine.[2],[3],[4],[5] The physiological laxity of the ligaments around the CV junction may be the underlying predisposing factor for rotatory subluxation. The presence of a torticollis in a child should arouse suspicion of rotatory atlantoaxial subluxation, particularly when there is a recent history of recent throat infection or trauma.[1]
Fielding and Hawkins classified atlantoaxial rotatory fixation into 4 types depending on the degree of atlantodental distance.[2] In Type I, the rotatory subluxation is associated with normal atlantodental interval. In Type II and Type III, the rotatory subluxations are associated with 3 to 5 mm and more than 5 mm of anterior displacement of the atlas respectively. Type IV rotatory subluxation is associated with posterior shift of the atlas due to failure of the dens.[2] The Type I variety is the commonest and the most benign form of rotatory subluxation, probably because the transverse ligament is intact. The diagnosis of atlantoaxial rotatory subluxation requires a high degree of suspicion based on the signs and symptoms. A CT scan of the atlantoaxial complex is most valuable for demonstrating the anatomy and a 3D-CT scan provides more direct visualization of the abnormal anatomy.[6] When diagnosed early, most patients respond well to a conservative treatment with cervical collar and bed-rest.[1] Surgical intervention is advised when conservative treatment fails to achieve reduction or is followed by a recurrence of the deformity.[2]
References
| 1. | Philips WA, Hensinger RN. The management of rotatory atlanto - Axial subluxation in children. J Bone Joint Surg (Am) 1989;71:664-8. Back to cited text no. 1 |
| 2. | Fielding JW, Hawkins RJ. Atlanto-axial rotatory fixation. J Bone Joint Surg 1977;59A:37-44. Back to cited text no. 2 |
| 3. | Dhaon BK, Jaiswal A, Nigam V, Jain V. Atlantoaxial rotatory fixation secondary to tuberculosis of occiput: A case report. Spine 2003;28:E203-5. Back to cited text no. 3 [PUBMED] [FULLTEXT] |
| 4. | Akpinar G, Tekkok IH, Sumer M. Grisel's syndrome: A case of potentially lethal spinal cord injury in the adult. Br J Neurosurg 2002;16:592-6. Back to cited text no. 4 [PUBMED] |
| 5. | Behari S, Jain VK, Phadke RV, Banerji D, Kathuria M, Chhabra DK. C1-C2 rotary subluxation following posterior stabilization for congenital atlantoaxial dislocation. Neurol India 2000;48:164-9. Back to cited text no. 5 [PUBMED] [FULLTEXT] |
| 6. | Scapinelli R. Three-dimensional computed tomography in infantile atlantoaxial rotatory fixation. J Bone Joint Surg Br 1994;76-B:367-70. Back to cited text no. 6 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04090f1.jpg]
[ni04090f2.jpg]
|

{kind=link}
{kind=link}