
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 275-276
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 275-276
Letter To Editor
Recurrent cerebral venous and peripheral arterial thrombosis
Alexander Mathew , Joseph Mathew , Gnanamuthu Chandran , Vaid Urvashi
Department of Neurological Sciences, Christian Medical College, Vellore - 632004
Correspondence Address:Department of Neurological Sciences, Christian Medical College, Vellore - 632004
mathew_koleth@hotmail.com
Code Number: ni04093
Sir,
Hereditary thrombophilia is caused by a variety of inherited disorders, which result in a familial tendency to recurrent thrombosis usually manifesting at an early age. Patients generally present with venous thrombosis, and arterial thrombosis if present, is most often due to atherosclerosis. However, in young individuals with arterial thrombosis, lacking recognized risk factors for atherosclerosis, studies have shown the prevalence of a hypercoagulable state to be 12 to 40 % (low levels of Protein C, Protein S, or antithrombin III, or the presence of lupus anticoagulant).[1] The occurrence of a venous and an arterial thrombosis simultaneously is an uncommon event, even in the presence of an underlying prothrombotic state. We present an unusual case of a young girl who presented with arterial and then venous thrombosis.
A 16-year-old girl presented to the emergency room of our hospital with a 3-day history of severe headache, vomiting and progressive visual loss. At the age of 14, she had developed a non-healing ulcer on her right foot, and three months later developed claudication of both lower limbs. She was evaluated for the same at another hospital and was found to have bilateral femoral artery thrombosis. She initially underwent a thrombectomy and ilio-femoral bypass, but subsequently developed gangrene and underwent bilateral above knee amputations. She was started on unfractionated heparin, but developed cavernous sinus thrombosis while on treatment, which resolved with higher doses of heparin. A complete thrombotic work-up was not done at that time but the bleeding time and the platelet count were normal. She was discharged from the hospital on oral anticoagulants and subsequently attended a rehabilitation clinic where limb prostheses were fitted. Anticoagulation was discontinued after six months and she was put on aspirin. She remained well for over a year until she developed her present symptoms.
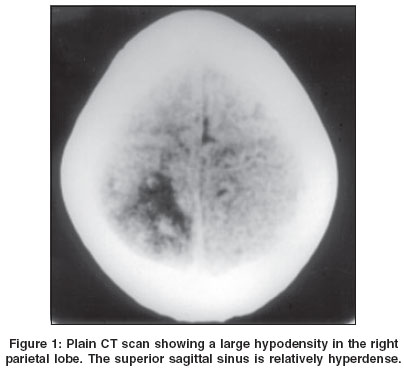
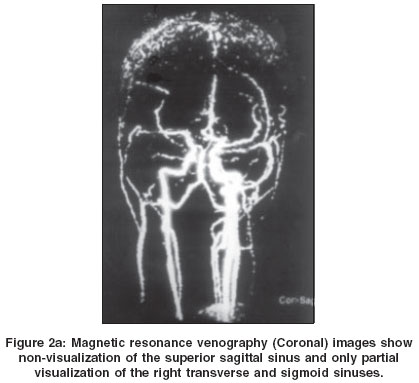
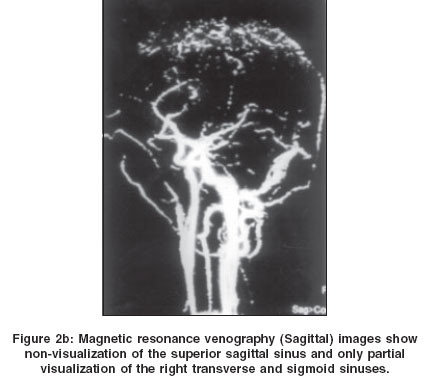
At presentation, she was afebrile, irritable and uncooperative, had bilateral papilledema with no lateralizing or meningeal signs. A contrast enhanced CT scan of the brain revealed evidence of dural sinus thrombosis with bilateral parieto-occipital hypo densities [Figure - 1]. Magnetic resonance venography confirmed the presence of sagittal and transverse sinus thrombosis [Figure - 2]a and [Figure - 2]b.
Baseline coagulation profile was normal and she was started on unfractionated heparin infusion and anti-edema measures. Despite being on heparin, she worsened over the next two days and developed bilateral proptosis and chemosis suggestive of cavernous sinus thrombosis. Her activated partial thromboplastin time was not prolonged even with 20 units of heparin per kilogram body weight, per hour. The possibility of antithrombin III deficiency was considered and she was started on low molecular weight heparin with which her symptoms and signs resolved rapidly over the next two days. She was subsequently started on oral anticoagulants and discharged.
Protein C, Protein S and antithrombin III could not be assessed before she was started on anticoagulants due to technical reasons. DNA analysis was negative for Factor V Leiden and prothrombin mutations, but she was found to be heterozygous for the methylenetetrahydrofolate reductase C667T mutation.
Patients with hereditary thrombophilia generally present with venous thrombosis. The occurrence of a venous and an arterial thrombosis simultaneously is an uncommon event. D Nagaraja et al reported three patients (two below 40 years of age) in whom simultaneous thrombosis of cortical veins and sinuses and major cerebral arteries was observed. The coagulation profile was not assessed and the diagnosis was based on partial autopsies.[2]
Our patient did not respond to conventional heparin but responded to low molecular weight heparin, suggesting an antithrombin III deficiency which we were unfortunately unable to confirm by laboratory tests. She was found to be heterozygous for methylenetetrahydrofolate reductase C667T mutation, which causes homocysteinemia.[3],[4],[5] Elevated levels of homocysteine could explain the patient′s thrombophilic state and the apparent antithrombin III deficiency. Since she was positive for the C667T mutation, we concluded that homocysteinemia was the probable cause of her thrombophilia. Stopping anticoagulants and replacing them with anti-platelet drugs could be harmful in the absence of a definitive diagnosis, as in our patient. Thrombophilic disorders of unknown etiology should be managed only with anticoagulants.
References
| 1. | Miljic P, Rolovic Z, Elezovic I, Antunovic P, Stanojevic M, Colovic M. Hereditary deficiency of Antithrombin III, Protein C, Protein S & Factor XII in 121 patients with venous or arterial thrombosis. Srp Arti Celok Lek 1999;127:21-7. Back to cited text no. 1 |
| 2. | Nagaraja D, Taly AB, Shankar SK. Simultaneous cerebral arterial and venous thrombosis. JAPI J Assoc Physicians India 1990;38:325-6. Back to cited text no. 2 |
| 3. | Graham IM, Daly LE, Refsum HM, Robinson K, Brattstrom LE, Ueland PM et al. Plasma homocysteine as a risk factor for vascular disease. The European Concerted Action Project. JAMA 1997;277:1775-81. Back to cited text no. 3 [PUBMED] |
| 4. | D'Angelo A, Selhub J. Homocysteine and thrombotic disease. Blood 1997;90:1-11. Back to cited text no. 4 |
| 5. | Clarke R, Daly LE, Robinson K, Naughton E, Cahalene S, Fowler B et al. Hyperhomocysteinemia: An independent risk factor for vascular disease. N Engl J Med 1991;17:1149-55. Back to cited text no. 5 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04093f2a.jpg]
[ni04093f2b.jpg]
[ni04093f1.jpg]
|

{kind=link}
{kind=link}
{kind=link}