
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 278-279
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 278-279
Letter To Editor
Calvarial tuberculosis
Rajmohan BP, Anto Dominic , Alappat Jacob P
Department of Neurosurgery, Medical College, Calicut, Kerala
Correspondence Address:Department of Neurosurgery, Medical College, Calicut, Kerala
cmcalumni@eth.net
Code Number: ni04095
Sir
Calvarial tuberculosis is a rare manifestation of extrapulmonary tuberculosis with few reports in the literature.[1],[2]
A 16-year-old girl from a middle class family presented with a left parietal scalp swelling noticed incidentally three months prior to admission after a minor trauma. The swelling was 5 cm x 4cm in size, was non-tender and there were no signs of inflammation. The scalp over the swelling was normal. There was an impulse on coughing and a palpable calvarial defect with everted bony edges. General physical and routine hematological examination revealed no abnormality. Erythrocyte sedimentation rate was 22 mms in the first hour. X-ray of the skull revealed a lytic area in the left parietal bone with sclerosis of the edges.
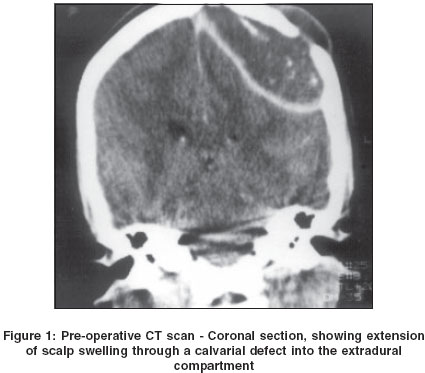
Computerized tomogram of the head showed an encapsulated lesion with calcified foci communicating between the intracranial and extracranial compartments eroding the inner and outer tables of the skull near the left parietal eminence [Figure - 1]. The margins of the lesion exhibited minimal contrast enhancement. Magnetic resonance imaging of the brain showed a hypointense and intermediate signal lesion over the left parietal lobe extradurally in T1 weighted images with intermediate to hyperintense signals on T2 weighted images, extending medially up to the superior sagittal sinus.
The lesion was exposed after taking an incision around the swelling. The whole lesion was excised piecemeal, laterally up to the normal bone margin. The contents of the lesion resembled the cheesy material of an epidermoid cyst. The capsule of the lesion was peeled off completely from the dura. The defect in the calvarial bone was repaired with the help of iliac bone graft. The histopatholgical examination confirmed that the lesion was tuberculous osteomyelitis. The patient was treated with antituberculous drugs. A repeat CT head scan confirmed that the grafts had fused. HIV status was checked and was found to be negative. The patient recovered clinically and gained weight.
Isolated calvarial tuberculosis is rare[3] but can be seen in association with pulmonary tuberculosis, tuberculous osteomyelitis involving other bones, cervical lymphadenitis, renal and intestinal tuberculosis. The frontal and parietal bones, having greater area of diploic space and cancellous bone are more vulnerable.[4] The tubercular process reaches the vault bones possibly through the blood stream. Concentrically placed fibroblasts proliferate and encircle the tubercular granulation tissue and prevent its extension through the bone; which when deficient, extension occurs through the inner or outer or both tables.[5] Sutures are not a strong barrier to spread but the dura usually prevents intradural extension. An extensive area of destruction occurs before clinical presentation.
The radiological picture can vary, with either an osteolytic or sclerotic variety being seen; the osteolytic type itself can be circumscribed or of the spreading type.[2] The CT picture of tuberculous osteomyelitis is not very specific, with pyogenic osteomyelitis, calvarial metastases, myeloma, hemangioma, giant cell tumor or even an aneurysmal bone cyst and Langerhans cell histiocytosis forming the differential diagnoses.[5]
The criterion for diagnosis is isolation of tubercle bacilli, which most of the time is not possible, as in our case. In the absence of this, histological features of caseous granuloma are often the only clue, along with the radiological features.[6] On many occasions, there may not be supporting evidence of extracalvarial tuberculosis or raised erythrocyte sedimentation rate.[5] Clinical and radiological response to specific anti-tuberculous chemotherapy is usually good.[3]
References
| 1. | Strauss DC. Tuberculosis of flat bones of the vault of the skull. Surg Gynaecol Obstet 1933;57:384-98. Back to cited text no. 1 |
| 2. | Barton CJ. Tuberculosis of the vault of the skull. Br J Radiol 1961;34:286-90. Back to cited text no. 2 [PUBMED] |
| 3. | Jadhav RN, Palande DA, et al. Calvarial tuberculosis. Neurosurgery 1999;45:1345-50. Back to cited text no. 3 |
| 4. | Meng CM, WU YK. Tuberculosis of the flat bones of the vault of the skull. J Bone Joint Surg 1942;34:341-53. Back to cited text no. 4 |
| 5. | Gupta PK, Kolluri VRS, Chandramouli BA, et al. Calvarial tuberculosis: A report of two cases. Neurosurgery 1989;25:830-3. Back to cited text no. 5 |
| 6. | Patankar T, Varma R, et al. Radiographic findings in tuberculosis of the calvarium Neuroradiology 2000;42:518-21. Back to cited text no. 6 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04095f1.jpg]
|

{kind=link}