
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 279-279
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 279
Letter To Editor
Vertebrobasilar dolichoectasia presenting as lower cranial nerve palsy
Panda S, Goyal V, Gupta V, Singh S, Srivastava T, Padma MV, Behari M
Department of Neurology, All India Institute of Medical Sciences, New Delhi - 110029
Correspondence Address:Department of Neurology, All India Institute of Medical Sciences, New Delhi - 110029
drvinaygoyal@hotmail.com
Code Number: ni04096
Sir
Intracranial arterial dolichoectasia is characterized by enlargement, tortuosity or elongation of major arteries at the base of the brain. It usually involves distal vertebral arteries, basilar artery or distal internal carotid artery. Vertebrobasilar dolichoectasia (VBDE) is relatively rare. It generally manifests as compression of cranial nerves or the brainstem, ischemic stroke or transient ischemic attacks (TIA) and rarely as intracerebral hemorrhage.[1],[2] We report here a case of VBDE presenting with lower cranial nerve palsy.
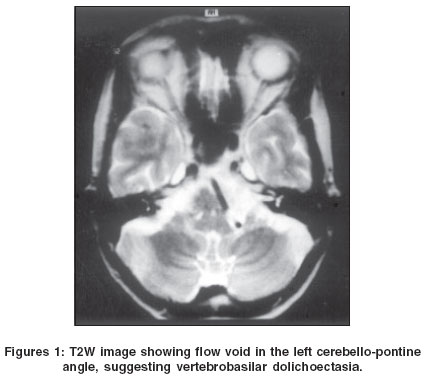
A 55-year-old lady having moderate hypertension presented with history of insidious onset, progressive hoarseness of voice and dysphagia for last one year. Neurological examination revealed that the uvula was deviated to the right side. Palatal movements, sensation of touch in the throat and gag reflex was diminished on the left side. Her voice was of low volume, hoarse and husky without any nasal twang. Deep tendon reflexes were brisker and plantar was extensor on the left side. The rest of the examination revealed no abnormality. Non-contrast computerized tomogram (NCCT) of head showed evidence of ectatic vertebrobasilar artery. MRI brain [Figure - 1] showed evidence of tortuosity of the distal vertebral and basilar arteries. There was mass effect upon the medulla by these ectatic arteries causing flattening of the left medullary pyramid. In addition, there were periventricular white matter changes and a small infarct in the right cerebral peduncle.
The most common site of dolichoectasia is the vertebrobasilar system. The basilar artery is judged elongated if at any point along its course, it lies lateral to the margin of the clivus or dorsum sellae or if its bifurcation is above the plane of the suprasellar cistern, and the artery is considered ectatic if the diameter of the artery is greater than 4.5 mm. The factors responsible for the development of dolichoectasia are unclear. The degeneration of the vascular wall due to atherosclerosis alone or in association with arterial hypertension is suggested as the pathogenetic factor. However, others consider VBDE to be a congenital vascular anomaly on the basis of histological observations of defects in the internal elastic lamina and thinning of the media secondary to smooth muscle atrophy.[3] Also, VBDE is suggested to be a component of generalized ectasia of the intracranial vessels[4] and is associated with ectasia in other vascular territories and with aneurysm of the abdominal aorta.[4] Rarely, it has been documented in Fabry′s disease.[5]
VBDE has been identified to produce cranial nerve palsy due to compression of the brainstem, ischemic stroke, cerebral hemorrhage and subarachnoid hemorrhage. Rarely, they are asymptomatic. We did not find any report of IXth or Xth cranial nerve involvement due to VBDE except a case of lower cranial nerve palsy due to compression of the medulla oblongata by tortuous vertebral artery reported by Hongo et al.[6]
Lower cranial nerve involvement in the present patient is a manifestation of VBDE, with compression of the left IX and X cranial nerves during the extra-axial course. The asymmetrical ipsilateral pyramidal signs were either due to gross distortion of the left medullary pyramid or due to infarct in the right cerebral peduncle. The associated evidence of periventricular white matter changes supports the probable mechanism of atherosclerosis responsible for the development of VBDE. Our patient did not agree for surgery, therefore the possible response to decompressive surgery could not be established.
References
| 1. | Baquero M, Yaya HR. Vertobasilar dolichoectasia. Rev Neurol 1998;26:143-8. Back to cited text no. 1 |
| 2. | Rautenberg W, Aulich A, Rother J, et al. Stroke and dolichoectatic intracranial arteries. Neurol Res 1992;14:201-3. Back to cited text no. 2 [PUBMED] |
| 3. | Hegedus K. Ectasia of the basilar artery with special reference to possible pathogenesis. Surg Neurol 1985;24:463-9. Back to cited text no. 3 [PUBMED] |
| 4. | Hulten GIL, Lofstedt S, Von Reis G. Observations on generalized arteriectasis. Acta Med Scand 1959;163:125-30. Back to cited text no. 4 |
| 5. | Mitsias P, Levine SR. Cerebrovascular complications of Fabry's disease. Ann Neurol 1996;40:8-17. Back to cited text no. 5 [PUBMED] |
| 6. | Hongo K, Nakagawa H, Morota N, Isobe N. Vascular compression of the medulla oblongata by vertebral artery: Report of two cases. Neurosurg 1999;45:907-10. Back to cited text no. 6 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04096f1.jpg]
|

{kind=link}