
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 280-281
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 280-281
Letter To Editor
Uncommon manifestations of neurosarcoidosis
Modi M, Bhatia R, Jain R, Lal V, Radotra BD, Aggarwal A
Departments of Neurology, Neurosciences Centre, AIIMS, New Delh
Correspondence Address:Departments of Neurology, Neurosciences Centre, AIIMS, New Delh
rohitbhatia71@yahoo.com
Code Number: ni04097
Sir
Neurological manifestations in sarcoidosis, a multisystem granulomatous disease with enhanced cellular immune process at the site of disease activity, occur in 5% to 6% patients with sarcoidosis.[1],[3]
A 52-year-old male developed left-sided lower motor neuron type of facial nerve palsy, which responded to steroid therapy. Two months later, the patient developed dysarthria, difficulty in swallowing and nasal regurgitation of fluids. He gave history of cough, expectoration and wheezing with seasonal exacerbations, responding to bronchodilators and steroids for the past 30 years. He was treated with long-term steroids for allergic bronchopulmonary aspergillosis (ABPA).
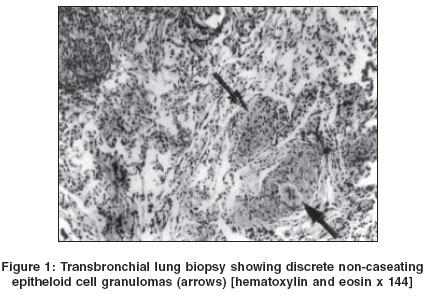
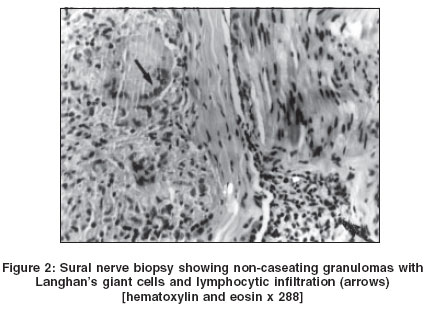
Examination revealed residual left VII nerve paresis with evidence of right-sided IX and X nerve palsy and partial involvement of right XI nerve. There was pansensory loss on the trunk involving the D5 to D8 region on the left side. The ankle reflexes were absent bilaterally with mild impairment of touch, joint position and vibration sensation in the upper and lower limbs in a glove and stocking distribution. Nerve conduction studies revealed evidence of symmetrical axonal sensorimotor neuropathy, predominantly involving the lower limbs. Transbronchial lung biopsy and nerve biopsy of the right sural nerve revealed non-caseating granulomas with giant cell formation consistent with the diagnosis of sarcoidosis [Figure - 1] and [Figure - 2]. The patient was initially treated with oral prednisolone in the dose of 1mg/kg/day for 4 weeks followed by gradual tapering to a dose of 10 mg every alternate day. Subsequently, chloroquine at a dose of 150 mg b.i.d/day was added with regular monitoring of visual impairment. The patient showed remarkable clinical improvement in bulbar symptoms and truncal pain within 2 weeks of starting the therapy, with gradual improvement thereafter.
Neurosarcoidosis can manifest in myriad ways including cranial neuropathy, aseptic meningitis, mass lesions, encephalopathy, vasculopathy, seizures, psychiatric manifestations, hydrocephalus, hypothalamic pituitary disorders, myelopathy, peripheral neuropathy and myopathy.[3],[4],[5],[6] The mode of onset of neurosarcoidosis is variable, but it is usually subacute to chronic. Acute onset neurological disease usually presents with isolated cranial neuropathies and aseptic meningitis, while patients with a chronic onset usually present with parenchymal involvement, hydrocephalus or peripheral nervous system manifestations.[7] Cranial neuropathy is the most common manifestation of neurosarcoidosis occurring in up to 75% of the patients.[8] The facial nerve is the most commonly affected cranial nerve and is involved in up to 50% of neurosarcoidosis patients.[9] Though commonly unilateral, bilateral facial palsy can occur simultaneously or sequentially in approximately one-third of the patients.[10] Other cranial nerves, especially the IX and X are less commonly affected.[9] The pattern of non-cranial peripheral neuropathy includes patchy neuropathy or mononeuritis, a component of which may be an `intercostal neuritis′ with numb patches on the trunk (as seen in the present case), acute Guillaine-Barre syndrome (GBS), and chronic sensorimotor, motor or pure sensory neuropathies.[3],[11],[12] Of these, chronic symmetric axonal sensorimotor polyneuropathy is most commonly observed.[12] A combination of multiple cranial and non-cranial neuropathies was also observed in our patient. Sensorimotor neuropathy has been attributed to epineural and perineural granulomas with an associated granulomatous vasculitis, producing an axonal degeneration with associated demyelination.[12],[13] Although non-caseating granulomas are rarely observed in nerve biopsy samples,[13] the sural nerve biopsy in our patient revealed these characteristic changes [Figure - 2].
Unlike pulmonary sarcoidosis where a period of observation is recommended for mild and asymptomatic cases, neurosarcoidosis should always be treated.[14] Treatment decisions are governed by disease location, clinical severity, time course and morbidity of treatment. Corticosteroids are the cornerstone of the therapy for neurosarcoidosis. Steroid therapy is usually started at a high dose and after achieving a clinical response, the dose is gradually tapered.[14] Alternative therapeutic agents are indicated in patients with steroid side-effects or lack of response to treatment or in cases where steroids are contraindicated. These include cyclosporine, azathioprine, hydroxychloroquine, chloroquine and radiation therapy.[15] Chloroquine and hydroxychloroquine have been found to be effective in controlling neurosarcoidosis in patients who fail to respond to corticosteroids or develop serious side-effects, with no evidence of ocular toxicity during the treatment.[16] Clinical manifestations are the best predictors of the course and prognosis in patients with neurosarcoidosis.[16] Cranial neuropathies and aseptic meningitis carry the best prognosis with recovery in up to 90% of cases.[9],[10] Approximately 32% of the patients with neurosarcoidosis, especially those with cranial neuropathies, relapse after the initial neurological episode.[11] Patients with parenchymal disease generally have a prolonged disease course with significant morbidity. Among the peripheral nervous system manifestations, polyradiculitis and acute myopathy tend to respond well to steroids compared to the slowly progressive peripheral neuropathy and myopathy.[10]
References
| 1. | John CJ, (Ed). Tenth International Conference on sarcoidosis and other granulomation disorders. Ann NY Acad Sc 1986;465:1. Back to cited text no. 1 |
| 2. | Chapelan C, Uzzar B, Piette JCh, et al. Sarcoidosis in Internal Medicine: A cooperative study of 554 cases. Ann Med Intern 1984;135:125-31. Back to cited text no. 2 |
| 3. | Stern BJ, Krumholz A, Johns C. Sarcoidosis and its neurological manifestations. Arch Neurol 1985;42:909-17. Back to cited text no. 3 |
| 4. | Wiederholt WC, Siekert RG. Neurological manifestations of sarcoidosis. Neurology 1965;19:1147-54. Back to cited text no. 4 |
| 5. | Pentland B, Mitchell JD, Cull RE, Ford MJ. Central nervous system Sarcoidosis. Quart J Med 1985;56:457-65. Back to cited text no. 5 [PUBMED] |
| 6. | Younger DS, Hayo AP, Brust JC, Rawland LP. Granulomatous angiitis of the brain. An inflammatory reaction of diverse etiology. Arch Neurol 1988;45:514-8. Back to cited text no. 6 |
| 7. | Luke RA, Stern BJ, Krumholz A, et al. Neurosarcoidosis: The long term clinical course. Neurology 1987;37:461-3. Back to cited text no. 7 [PUBMED] |
| 8. | Delaney P. Neurologic manifestations in Sarcoidosis: Review of literature, with report of 23 cases. Ann Intern Med 1977;87:336-45. Back to cited text no. 8 [PUBMED] |
| 9. | Chapelon C, Ziza JM, Piette JC, et al. Neurosarcoidosis: Sign, course and treatment in 35 confirmed cases. Medicine (Baltimore) 1990;69:261-76. Back to cited text no. 9 [PUBMED] |
| 10. | Oksanen V. Neurosarcoidosis: Clinical presentation and course in 50 patients. Acta Neurol Scand 1986;73:283-90. Back to cited text no. 10 [PUBMED] |
| 11. | Scott TF. Neurosarcoidosis. Progress and clinical aspects. Neurology 1993;43:8-12. Back to cited text no. 11 [PUBMED] |
| 12. | Zuniga G, Ropper AH, Frank J. Sarcoid peripheral neuropathy. Neurology 1991;41:1558-61. Back to cited text no. 12 [PUBMED] |
| 13. | Nemni R, Galassi G, Cohen M, et al. Symmetric sarcoid polyneuropathy: Analysis of sural nerve biopsy. Neurology 1981;31:1212-23. Back to cited text no. 13 |
| 14. | Hunninghake GW, Gilbert S, Pueringer R, et al. Outcome of the treatment of Sarcoidosis. Ann J Respir care Med 1994;149:893-8. Back to cited text no. 14 [PUBMED] |
| 15. | Agbogu BN, Stern BJ, Sewell C, et al Therapeutic considerations in patients with refractory neurosarcoidosis. Arch Neurol 1995;52:875-9. Back to cited text no. 15 |
| 16. | Sharma OP. Effectiveness of chloroquine and Hydroxychloroquine in treating selected patients with sarcoidosis with Neurological involvement. Arch Neurol 1998;55:1248-54. Back to cited text no. 16 [PUBMED] [FULLTEXT] |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04097f2.jpg]
[ni04097f1.jpg]
|

{kind=link}
{kind=link}