
|
Neurology India
Medknow Publications on behalf of the Neurological Society of India
ISSN: 0028-3886 EISSN: 1998-4022
Vol. 52, Num. 2, 2004, pp. 283-284
|
Neurology India, Vol. 52, No. 2, April-June, 2004, pp. 283-284
Letter To Editor
Acute inflammatory demyelinating polyneuropathy in patients with pregnancy
Goyal V, Misra BK, Singh S, Prasad K, Behari M
Department of Neurology, All India Institute of Medical Sciences, New Delhi - 110029
Correspondence Address:Department of Neurology, All India Institute of Medical Sciences, New Delhi - 110029
drvinaygoyal@ hotmail.com
Code Number: ni04100
Sir
Acute inflammatory demyelinating polyneuropathy (AIDP) is an acute monophasic type of demyelinating neuropathy, with symmetrical muscle weakness areflexia and ascending paralysis. AIDP has been reported during all the three trimesters of pregnancy[1] and in the post-partum period.[2] It is known to worsen during the post-partum period due to a rapid increase in delayed type hypersensitivity during this period. Relapse during successive pregnancies has been reported.[3] Though the incidence of AIDP in pregnancy is similar to that in the normal population,[4] only 50 cases of AIDP during pregnancy have been reported.[5] The occurrence of the disease in the third trimester presents a high maternal risk because of respiratory complications and risk of premature delivery. We successfully managed a patient of AIDP during pregnancy who showed remarkable recovery following delivery.
A 25-year-old primigravida with 26 weeks of pregnancy presented with acute onset progressive weakness of all four limbs for 10 days and diarrhea with mild fever 2 weeks prior to limb weakness.
Examination showed anemia, pregnancy of 26 weeks, and normal cranial nerves, power of 1/5 in the upper limbs, and 1/5 in proximal and 3/5 in distal muscles of lower limbs. There was generalized hypotonia and areflexia with bilateral flexor planter reflex. There was no sensory impairment or bladder and bowel involvement. During hospitalization she developed bilateral facial weakness, dysphasia and dysarthria with worsening of the limb power to 0/5 on the 15th day. Her respiratory effort weakened requiring intubation and ventilatory support on the 34th day due to inability to maintain oxygen saturation. Tracheostomy was done after the 51st day of illness. Obstetricians were consulted throughout her hospital stay. She delivered a healthy baby of 2.4 kg at 37 weeks of gestation and needed outlet forceps with right mediolateral episiotomy to reduce the duration of the second stage of labor. The baby had two rounds of cord around the neck but cried immediately. The baby was healthy and had no signs of birth asphyxia. The postnatal period was uneventful. Following delivery, the patient showed steady improvement and was weaned off from the ventilator on the 20th postnatal day (94th day of illness). She required intragastric tube feeding up to the 98th day of illness. The patient was treated with plasmapharesis (PP), within 24 hours of admission, consisting of five cycles of PP on alternate days with removal of 750 ml plasma and replacement of 300 ml of 5% albumin solution each time. She was discharged from the hospital after 14.5 weeks when she was partly but significantly dependent for activity of daily life. Her power was 3/5 in the upper limbs and 2/5 in both the lower limbs with generalized areflexia.
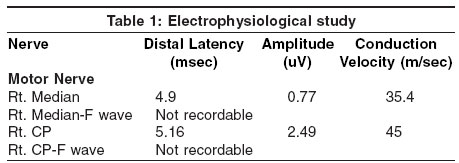
The results of the electrophysiological study done on the day of admission, are shown in [Table - 1]. The common peroneal nerve had evidence of conduction block as evidenced by a significant reduction in the amplitude of compound muscle action potential.
F waves could not recorded in any nerves. Sensory nerve conduction study was within normal limits.
AIDP is a disorder of presumed autoimmune pathogenesis. It is known to develop at all ages and is reported in pregnancy as well. Reports of treatment of AIDP in pregnancy with IVIG[5],[6] and PP[4],[1] are available in the literature. Our case was unique in the way that we treated this case with PP in the second trimester of pregnancy. IVIG and PP are the treatment of choice for AIDP.[7] IVIG is preferred due to lesser complications as compared to PP. Plasmapharesis has been done in pregnancy for both neurological and non-neurological disorders. Only a single report of AIDP in pregnancy being treated with PP is available in the literature.[1] The case we are reporting had AIDP in the second trimester. It is well known that AIDP may worsen in the third trimester of pregnancy just as this patient also worsened. She was treated with PP but she continued to worsen and required ventilatory support. Maintaining vitals, adequate ventilatory support without any complications and termination of pregnancy (by delivery) helped her to recover faster.
References
| 1. | Zeeman GG. A case of acute inflammatory demyelinating polyradiculoneuropathy in early pregnancy. Am J Perinatol 2001;18:213-5 . Back to cited text no. 1 [PUBMED] |
| 2. | Gautier PE, Pierre PA, Van Obbergh LJ, Van Steenberge A. Guillain-Barre syndrome after obstetrical epidural analgesia. Reg Anesth 1989;14:251-2. Back to cited text no. 2 [PUBMED] |
| 3. | D'Ambrosio G, De Angelis G. Syndrome de Guillain-Barre au cours de la grossesse. Ren Neurol (Paris) 1985;141:33. Back to cited text no. 3 |
| 4. | Clifton ER Gullien Barry syndrome, pregnancy & plasmapharesis. J Am Osteopath Assoc 1992;92:1279-82. Back to cited text no. 4 |
| 5. | Yamada H, Noro N, Kato ME, et al. Massive IV Immunoglobulin in pregnancy complicated by GB. Syndrome. Euro J Obs & Gynae & Reproductive Bio 2001;97:101-4. Back to cited text no. 5 |
| 6. | Breuer GS, Morali G, Finkelstein Y, Halevy J. A pregnant woman with hepatitis A and Guillain-Barre. J Clin Gastroenterol 2001;32:179-80. Back to cited text no. 6 |
| 7. | Van der Meche FGA, Schimitz PIM, Dutch Guillian-Barre Study Group: A randomized trial comparing intravenous immunoglobin and plasma exchange in Guillian-Barre syndrome. N Eng J Med 1992;326:1123-9. Back to cited text no. 7 |
Copyright 2004 - Neurology India
The following images related to this document are available:
Photo images
[ni04100t1.jpg]
|

{kind=link}